Wed, May 27, 2026
Volume 19, Issue 2 (Summer & Autumn 2022)
ASJ 2022, 19(2): 73-78 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Gohila G, Valli S. Clinical Significance of Superficial Brachial Artery and High Division of Brachial Artery. ASJ 2022; 19 (2) :73-78
URL: http://anatomyjournal.ir/article-1-307-en.html
URL: http://anatomyjournal.ir/article-1-307-en.html



1- Department of Anatomy, K.A.P. Viswanatham Govt Medical College, Tamil Nadu, India.
2- Department of Anatomy,Tirunelveli Govt Medical College,Tamil Nadu, India.
2- Department of Anatomy,Tirunelveli Govt Medical College,Tamil Nadu, India.
Full-Text [PDF 1160 kb]
(652 Downloads)
| Abstract (HTML) (2244 Views)
Full-Text: (1413 Views)
1. Introduction
Brachial artery is the major artery of the upper extremity. The brachial artery originates at the lower border of the teres major muscle, as a continuation of the axillary artery. After medially movement to the humerus, brachial artery move anteriorly to the bone until it lies between the humeral epicondyles. Brachial artery divides into radial and ulnar arteries at the neck of the radius, about 1-cm distal to the elbow joint. The epidermis, deep fascia, and superficial fascia all are fully covered by the brachial artery. It is separated from the median cubital vein anteriorly at the elbow by the bicipital aponeurosis. Near the distal attachment of the corocobrachialis (middle of the arm), the median nerve crosses the brachial artery from the lateral to medial side. The brachial artery is related posteriorly to the long head of the triceps, the medial head of the triceps, coracobrachialis, and the brachialis. Biceps overlap the artery in the distal half of the arm, where the corocobrachialis and median nerve are located laterally to the artery proximally, the median cutaneous nerve of the forearm and the ulnar nerve run medially to the artery proximally, and the basilic vein and the median nerve lie distally. Two venae commitantes that are connected to the artery by oblique and transverse branches, run with the brachial artery [1]. Profunda brachii artery, nutrient artery to humerus, superior ulnar collateral artery, inferior ulnar collateral artery, deltoid artery, radial artery, and ulnar artery are the major branches of the brachial artery.
Embryonical development can be used to explain variations in the arteries of the upper extremity. Initial arrangement of arteries is regulated by ectodermal-mesenchymal interactions and extracellular matrix elements in the growing limb bud [2]. The variations in arteries are caused by a few inductive elements from the limb mesenchyme [3]. To avoid any difficulties during percutaneous arterial catheterization, anatomical knowledge of the abnormal branching pattern of the brachial artery is crucial. By placing a sphygmomanometer cuff in the arm, the blood pressure can be measured in the brachial artery. The cubital fossa is the site for collection of arterial blood samples from the brachial artery. The superficial brachial artery (SBA) in the arm is highly vulnerable to traumatic injuries, can be mistaken for a vein, and may cause incorrect drug administration that might result in gangrene and other consequences. Brachial artery has been used as a tool to assess endothelium function in obstetrics. When femoral access is not possible, brachial artery is used in cardiac ventriculography.
2. Materials and Methods
The current study was conducted from 2015 to 2016 on upper limb specimens of 30 adults which were prepared from the Institute of Anatomy, Madras Medical College. These specimens were obtained from embalmed human cadavers. The upper limbs with typical anatomical characteristics in both genders and body sides were included. Traumatized and deformed upper limb specimens with contractures were excluded from the study. To see the brachial artery and its branches, a dissection was performed after locating the brachial artery’s origin and its branches in the forearm. The bicipital aponeurosis located in cubital fossa was dissected, showing the terminal branches of the brachial artery [4]. The brachial artery course and its termination were assessed at lower border of the teres major muscle and intercondylar line (ICL) of humerus. The course and different variations of brachial artery termination were then recorded. Given that the study was observational, results were described using frequency and percentage.
3. Results
Out of 30 dissected upper limb specimens, 29( 96.7%) revealed normal course of brachial artery; the remaining specimen (3.3%) revealed SBA (Table 1) which runs superficially to the median nerve from medial to lateral side and naturally divided into radial and ulnar arteries at the neck of the radius (Figure 1).

 28 out of 30 specimens (93.3%) had the brachial artery terminated below the ICL (at the neck of the radius). In 2 specimens (6.7%), brachial artery divided into the radial and ulnar arteries above the level of the ICL (Table 2).
28 out of 30 specimens (93.3%) had the brachial artery terminated below the ICL (at the neck of the radius). In 2 specimens (6.7%), brachial artery divided into the radial and ulnar arteries above the level of the ICL (Table 2).

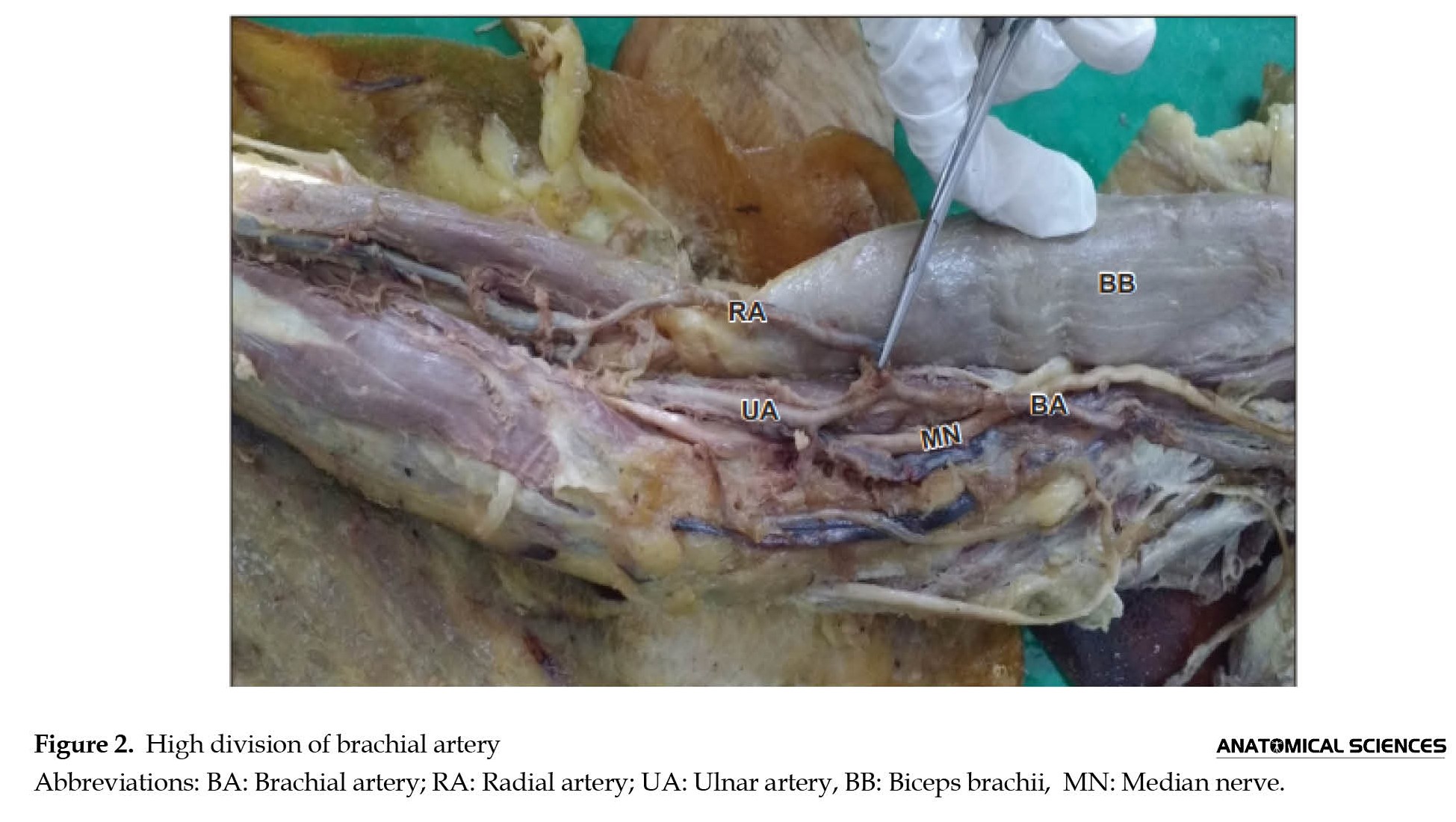
The division in one specimens occurred 2 cm above the ICL (Figure 2).
 In other specimen, the brachial artery was divided 5 cm above the ICL (Figure 3).
In other specimen, the brachial artery was divided 5 cm above the ICL (Figure 3).

4. Discussion
The branching pattern of the brachial arteries in the upper limbs are varied. These differences could result from a developmental defect during the formation of blood vessels, hemodynamic circumstances, or genetic predisposition.
Superficial brachial artery
Poirier in 1886 found SBA in 6% of the specimens [5]. Muller (1903) examined 100 upper limb specimens and observed that 1% had SBA [6]. In Linell et al.’s study in 1921, 34 upper limb specimens were dissected and it was found that 6% of brachial arteries ran superficially to the median nerve [7]. Miller in 1939 observed 3% SBA after dissecting 480 cadavers [8], while it was 5.7% in Mc Cormack et al.’ study [9], 5% in Kapur et al.’s study [10], 6% (from 50 upper limb specimens) in Patnaik et al.’s study [11], 5% (from 130 cadavers) in Kachlik et al.’s study [12], 1.9% (from 54 upper limb specimens) in Vatsala et al.’s study [13], and 5% (from 40 upper limb specimens) in Sathialakshmi et al.’s study [14]. The percentage of SBA in our study was 3.3% which is close to the findings of above-mentioned studies.
High division of brachial artery
High division in our study refers to the division of brachial artery above the ICL. Keen et al. in 1961 observed that 9% of brachial artery were divided above the ICL [15]. Karrlson & Niechajev in 1982 reported 10% high-division brachial artery [16]. After dissecting 10 cadavers, Priya et al. in 2012 found that 2(10%) had high division of brachial artery into radial and ulnar arteries just below the Profunda brachii muscle [17]. Varlekar et al. reported that 3 out of 96 upper limb specimens (6.25%) had a high brachial artery division [18]. Shuba et al. in 2013 found that 2% of the BA (from 95 upper limb specimens) were divided at the ICL [19]. According to Gujar et al. in 2014, 6% of specimens had high brachial artery division [20]. It was 4% (from 100 upper limb specimens) In Pundge et al.’s study in 2014 [21], 5% in Sathialakshmi et al.’s study in 2014 [14], 10% (from 40 cadavers) in Parimalasirkonda et al.’s study in 2016 [22], and 8% in Tsoucalas et al.’s study in 2020 [23]. In our study, 2 specimens (6.7%) had a high division of brachial artery; one 2 cm above the ICL and one 5 cm above the ICL. Before any invasive surgeries, knowledge of the high division of BA can be helpful. Brachial artery is employed in coronary angioplasty, embolectomy through arteriotomy, transbrachial access for renal artery intervention, and carotid artery stenting.
5. Conclusion
Due to the extensive clinical and radiological consequences, the brachial artery and its branching patterns have attracted the attention of many anatomists, surgeons, and radiologists. The brachial artery’s normal and abnormal morphologies in adult cadaver samples were examined in this paper. Clinical significance of SBA and the high division of the brachial artery is important in vascular procedures such as coronary artery bypass graft, orthopedic surgeries, and plastic and reconstructive surgery. SBA is more susceptible to traumatic injuries and cannulation. The superficial radial and ulnar arteries are exposed by elevating the radial forearm flap. Gangrene in fingers, hands, and forearms may be seen after an unintentional intra-arterial injection of medications. Before any invasive or interventional measures, the vascular pattern of the forearm can be determined using Doppler ultrasound and brachial artery angiography.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethical Committee of Madras Medical College (Code: ECR/270/Inst./TN/2013).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, methodology, software validation, and writing the original draft: G Gohila; Formal analysis and editing: S Valli; Review and editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank Sudha Seshayyan, director & head of the Department, Institute of Anatomy, Madras Medical College, The Tamil Nadu Dr. M.G.R. Medical University for her constant support and guidance during the research.
References
Brachial artery is the major artery of the upper extremity. The brachial artery originates at the lower border of the teres major muscle, as a continuation of the axillary artery. After medially movement to the humerus, brachial artery move anteriorly to the bone until it lies between the humeral epicondyles. Brachial artery divides into radial and ulnar arteries at the neck of the radius, about 1-cm distal to the elbow joint. The epidermis, deep fascia, and superficial fascia all are fully covered by the brachial artery. It is separated from the median cubital vein anteriorly at the elbow by the bicipital aponeurosis. Near the distal attachment of the corocobrachialis (middle of the arm), the median nerve crosses the brachial artery from the lateral to medial side. The brachial artery is related posteriorly to the long head of the triceps, the medial head of the triceps, coracobrachialis, and the brachialis. Biceps overlap the artery in the distal half of the arm, where the corocobrachialis and median nerve are located laterally to the artery proximally, the median cutaneous nerve of the forearm and the ulnar nerve run medially to the artery proximally, and the basilic vein and the median nerve lie distally. Two venae commitantes that are connected to the artery by oblique and transverse branches, run with the brachial artery [1]. Profunda brachii artery, nutrient artery to humerus, superior ulnar collateral artery, inferior ulnar collateral artery, deltoid artery, radial artery, and ulnar artery are the major branches of the brachial artery.
Embryonical development can be used to explain variations in the arteries of the upper extremity. Initial arrangement of arteries is regulated by ectodermal-mesenchymal interactions and extracellular matrix elements in the growing limb bud [2]. The variations in arteries are caused by a few inductive elements from the limb mesenchyme [3]. To avoid any difficulties during percutaneous arterial catheterization, anatomical knowledge of the abnormal branching pattern of the brachial artery is crucial. By placing a sphygmomanometer cuff in the arm, the blood pressure can be measured in the brachial artery. The cubital fossa is the site for collection of arterial blood samples from the brachial artery. The superficial brachial artery (SBA) in the arm is highly vulnerable to traumatic injuries, can be mistaken for a vein, and may cause incorrect drug administration that might result in gangrene and other consequences. Brachial artery has been used as a tool to assess endothelium function in obstetrics. When femoral access is not possible, brachial artery is used in cardiac ventriculography.
2. Materials and Methods
The current study was conducted from 2015 to 2016 on upper limb specimens of 30 adults which were prepared from the Institute of Anatomy, Madras Medical College. These specimens were obtained from embalmed human cadavers. The upper limbs with typical anatomical characteristics in both genders and body sides were included. Traumatized and deformed upper limb specimens with contractures were excluded from the study. To see the brachial artery and its branches, a dissection was performed after locating the brachial artery’s origin and its branches in the forearm. The bicipital aponeurosis located in cubital fossa was dissected, showing the terminal branches of the brachial artery [4]. The brachial artery course and its termination were assessed at lower border of the teres major muscle and intercondylar line (ICL) of humerus. The course and different variations of brachial artery termination were then recorded. Given that the study was observational, results were described using frequency and percentage.
3. Results
Out of 30 dissected upper limb specimens, 29( 96.7%) revealed normal course of brachial artery; the remaining specimen (3.3%) revealed SBA (Table 1) which runs superficially to the median nerve from medial to lateral side and naturally divided into radial and ulnar arteries at the neck of the radius (Figure 1).
The division in one specimens occurred 2 cm above the ICL (Figure 2).
4. Discussion
The branching pattern of the brachial arteries in the upper limbs are varied. These differences could result from a developmental defect during the formation of blood vessels, hemodynamic circumstances, or genetic predisposition.
Superficial brachial artery
Poirier in 1886 found SBA in 6% of the specimens [5]. Muller (1903) examined 100 upper limb specimens and observed that 1% had SBA [6]. In Linell et al.’s study in 1921, 34 upper limb specimens were dissected and it was found that 6% of brachial arteries ran superficially to the median nerve [7]. Miller in 1939 observed 3% SBA after dissecting 480 cadavers [8], while it was 5.7% in Mc Cormack et al.’ study [9], 5% in Kapur et al.’s study [10], 6% (from 50 upper limb specimens) in Patnaik et al.’s study [11], 5% (from 130 cadavers) in Kachlik et al.’s study [12], 1.9% (from 54 upper limb specimens) in Vatsala et al.’s study [13], and 5% (from 40 upper limb specimens) in Sathialakshmi et al.’s study [14]. The percentage of SBA in our study was 3.3% which is close to the findings of above-mentioned studies.
High division of brachial artery
High division in our study refers to the division of brachial artery above the ICL. Keen et al. in 1961 observed that 9% of brachial artery were divided above the ICL [15]. Karrlson & Niechajev in 1982 reported 10% high-division brachial artery [16]. After dissecting 10 cadavers, Priya et al. in 2012 found that 2(10%) had high division of brachial artery into radial and ulnar arteries just below the Profunda brachii muscle [17]. Varlekar et al. reported that 3 out of 96 upper limb specimens (6.25%) had a high brachial artery division [18]. Shuba et al. in 2013 found that 2% of the BA (from 95 upper limb specimens) were divided at the ICL [19]. According to Gujar et al. in 2014, 6% of specimens had high brachial artery division [20]. It was 4% (from 100 upper limb specimens) In Pundge et al.’s study in 2014 [21], 5% in Sathialakshmi et al.’s study in 2014 [14], 10% (from 40 cadavers) in Parimalasirkonda et al.’s study in 2016 [22], and 8% in Tsoucalas et al.’s study in 2020 [23]. In our study, 2 specimens (6.7%) had a high division of brachial artery; one 2 cm above the ICL and one 5 cm above the ICL. Before any invasive surgeries, knowledge of the high division of BA can be helpful. Brachial artery is employed in coronary angioplasty, embolectomy through arteriotomy, transbrachial access for renal artery intervention, and carotid artery stenting.
5. Conclusion
Due to the extensive clinical and radiological consequences, the brachial artery and its branching patterns have attracted the attention of many anatomists, surgeons, and radiologists. The brachial artery’s normal and abnormal morphologies in adult cadaver samples were examined in this paper. Clinical significance of SBA and the high division of the brachial artery is important in vascular procedures such as coronary artery bypass graft, orthopedic surgeries, and plastic and reconstructive surgery. SBA is more susceptible to traumatic injuries and cannulation. The superficial radial and ulnar arteries are exposed by elevating the radial forearm flap. Gangrene in fingers, hands, and forearms may be seen after an unintentional intra-arterial injection of medications. Before any invasive or interventional measures, the vascular pattern of the forearm can be determined using Doppler ultrasound and brachial artery angiography.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethical Committee of Madras Medical College (Code: ECR/270/Inst./TN/2013).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, methodology, software validation, and writing the original draft: G Gohila; Formal analysis and editing: S Valli; Review and editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank Sudha Seshayyan, director & head of the Department, Institute of Anatomy, Madras Medical College, The Tamil Nadu Dr. M.G.R. Medical University for her constant support and guidance during the research.
References
- Standring S. Gray’s anatomy: The anatomical basis of clinical practice. London: Churchill Livingstone Elsevier; 2008. [Link]
- Feinberg RN, Sherer GK, Auerbach R. The development of the vascular system. Karger, Basel. 1991; 14(3):136-48. [Link]
- Williams PL, Bannister LH, Berry MM, Collins P, Dyson M, Dussek JE, et al. Gray’s anatomy. London: Church Livingstone; 1999.
- Koshi R. Cunningham’s manual of practical anatomy. Oxford: Oxford ersity Press; 2017. [Link]
- Poirier P. [Tratado elemental de Anatomia Humaa (Spanish)]. Madrid: Administración de la Revista de Medicina y Cirugía Prácticas; 1908. [Link]
- Muller E. Beitrage zur morphologie des gefasssystem. Anatomische Hefte . 1903; 22:377-575. [DOI:10.1007/BF02267021]
- Linell EA. The distribution of the nerves in the upper limb, with reference to variabilities and their clinical significance. Journal of Anatomy. 1921; 55(2-3):79-112. [PMID]
- Miller RA. Observations upon the arrangement of auxiliary artery and brachial plexus. American Journal of Anatomy. 1939; 64(1):143-63. [DOI:10.1002/aja.1000640107]
- McCormack LJ, Cauldwell EW, Anson BJ. Brachial and antebrachial arterial patterns: A study of 750 extremities. Surgery, Gynecology & Obstetrics. 1953; 96(1):43-54. [PMID]
- Kapur V, Suri RK, Manik P, Dhir V. Surgical anatomy of the median nerve. Journal of the Anatomical Society of India. 2000; 49(1):92. [Link]
- Patnaik GVV, Kalsey G, Singla RK. Branching pattern of the brachial artery - A morphological study. Journal of Anatomical Society of India. 2002; 5(12):176-86. [Link]
- Kachlik D, Konarik M, Baca V. Vascular pattern of upper limb: An anatomical study with accent on superficial brachial artery. Bosnian Journal of Basic Medical Sciences. 2011; 11(1):4-10. [DOI:10.17305/bjbms.2011.2615] [PMID]
- Vatsala AR, Rajasekar HV, Angadi AV. Variation in the branching pattern of the brachial artery: A morphological and statistical study. International Journal of biomedical Research. 2013; 4(1):2920-3. [Link]
- Sathialakshmi V, Udaykumar, Felecia Ch, Sujatha N, SwayamJothi S. Variation of brachial artery and its branching pattern in India. Journal of Dental and Medical Sciences. 2014; 13(4):106-9. [DOI:10.9790/0853-1345106109]
- Keen JA. A study of the arterial variations in the limbs with special reference to the symmetry of vascular patterns. The American Journal of Anatomy. 1961; 108:241-61. [DOI:10.1002/aja.1001080303] [PMID]
- Karlsson S, Niechajev IA. Arterial anatomy of the upper extremity. Acta Radiologica: Diagnosis. 1982; 23(2):115-21. [DOI:10.1177/028418518202300206] [PMID]
- Priya G, Radhika Krishnan J, Sundarapandian S. Anatomy of an amorphic branching pattern of the brachial artery and its clinical complications: A cadaveric study. International Journal of Anatomical Sciences. 2012; 23(1):23-5. [Link]
- Varlekar P, Chavda H, Kubavat D, Nagar S, Saiyad SS, Lakhani C. Higher bifurcation of the brachial artery with a superficial course of the radial artery in the forearm: A case report. International Journal of Medical Science and Public Health. 2013; 2(3):703-6. [Link]
- Shubha R, Sudharsan Babu KG, Mekala D, Jeyanthi K, Lalitha C. An anatomical study of variations in the termination of the brachial artery: Embryological basis and clinical implications. Journal of Dental and Medical Sciences. 2018; 9(1):68-75. [Link]
- Gujar SM, Oza SG, Shekawat JP, Vikani SK, Prajapati. A study on the brachial artery and its clinical correlations. International Journal of Anatomy and Research. 2014; 2(1):208-12. [Link]
- Pundge S, Wadekar P, Gangane S, Sukre S. Branching pattern of brachial artery - A morphological study. International Journal of Healthcare and Biomedical Research. 2014; 2(4):90-9. [Link]
- Sirikonda P, Nalluri HB. An anatomical insight into high division of the brachial artery: A study in 40 cadavers. International Journal of Anatomy and Research. 2016; 4(1):1864-8. [DOI:10.16965/ijar.2015.353]
- Tsoucalas G, Eleftheriou A, Panagouli E. High bifurcation of the brachial artery: An embryological overview. Cureus. 2020; 12(2):1-4. [Link]
Type of Study: Original |
Subject:
Gross Anatomy
Received: 2021/12/16 | Accepted: 2022/07/2 | Published: 2022/07/1
Received: 2021/12/16 | Accepted: 2022/07/2 | Published: 2022/07/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
