Tue, Jul 8, 2025
Volume 15, Issue 1 (Winter & Spring 2018)
ASJ 2018, 15(1): 9-14 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Abbasi A, Jalilvand H, Jalilvand Karimi L, Akbarzade Baghban A. The Relationship Between Acceptable Noise Level and Initial Acceptance of Hearing Aid. ASJ 2018; 15 (1) :9-14
URL: http://anatomyjournal.ir/article-1-213-en.html
URL: http://anatomyjournal.ir/article-1-213-en.html


1- Department of Audiology, School of Rehabilitation, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Keywords: Acceptable noise level, Cognition, Hearing in noise, Hearing aid acceptance and commitment, Hearing loss, Hearing impaired behavior
Full-Text [PDF 482 kb]
(1611 Downloads)
| Abstract (HTML) (5219 Views)

Full-Text: (2504 Views)
1. Introduction
Hearing loss is beyond a personal problem. It affects patient’s life and can influence his/her relationship with the family, friends, and colleagues [1]. Fortunately, a significant improvement can be achieved in various aspects of life following the diagnosis of hearing loss and the rehabilitation via hearing aid [2, 3]. However, only a few patients with hearing impairments accept using hearing aids. Unfortunately, the usage of hearing aid is not mostly common among the patients with hearing impairments; for example, in the American countries, less than 25% of patients who are candidates for using hearing aids really attempt to use it.
This rate is even lower in the developing countries [4]. It made a group of researchers enthusiastic to study the factors affecting the acceptance and refusal of using hearing aids in such patients. According to the study by Nabelek et al., the main reason is attributed to the problem of amplified ambient noise [5]. In order to answer the question: “How much ambient noise can be bothersome enough to prevent a person from using hearing aid?” they designed and developed a practical speech test called Acceptable Noise Level (ANL) [6].
ANL evaluates the willingness of a listener to hear a continuous speech in the presence of background noise. To perform ANL, first patient’s most comfortable level (MCL) is determined by a speech signal; then, babble noise is added and the patient is asked to adjust it to the highest tolerable level while listening to the speech signal and the story. The obtained level is called the Background Noise Level (BNL). ANL in fact is MCL minus BNL. Practically, ANL is the lowest Signal-to-Noise Ratio (SNR) that a patient can put up with [7]. There is no association between ANL results and gender, hearing sensitivity, age, and speech “perception” in noise [8]. Generally ANL assumption is relied on the fact that some of the patients with hearing impairment do not accept hearing aids, which is the result of their inability to accept the background noise [7].
Since ANL could be a good predictor of this feature, the question is “Who is more successful in the full-time application of hearing aids and who can find it more enjoyable?” and relying on the answers, ANL can be considered as an useful and powerful advisory tool for hearing specialists in all of audiology clinics [6]. According to the realistic expectations, ANL can give audiologists a conception to figure out who needs more advice or who requires more advanced technologies such as directional microphones or assistive listening devices [9]. In other words, what type of patients can tolerate more background noise during a conversation? Briefly, patient’s ANL can give audiologists better and more reliable information to provide more accurate and successful hearing aid counseling.
Although there are many factors for the selection of hearing aid by patient, all of them are subjective and there is no objective measurement tool to assess hearing aid acceptance [9]. Also, the most important factor that influences hearing aid acceptance is patient’s personality and viewpoint in this regard, and according to the results of the current study, there was a significant relationship between the personality and ANL [9]. The main question of the current study was to evaluate the relationship between ANL and hearing aid acceptance in the patients.
Many studies were performed on the relationship between ANL and hearing aid satisfaction, but there was no study on the usage of ANL as the predictor of initial hearing aid acquisition. All studies were focused on the prediction of hearing aid benefits. The current research attempted to improve the rehabilitation given to the patients; authors hope it is useful to other researchers to provide a better understanding the reaction of patients to background noise in order to consider their hearing aid counseling and prescription, and also find out the reason of indifference in some patients with hearing aid acquisition, despite the best efforts the current study maid in hearing aid counseling. The main purpose of the study was to evaluate the relationship between the initial acceptance of hearing aid and individual’s ANL.
2. Materials and Methods
Study subjects
The current study performed on 60 patients with hearing loss who were the candidates for wearing hearing aid; they were assigned to 2 groups: the first group included 30 patients who accepted to take hearing aid and the second group compromised of 30 patients who refused to take hearing aid. The inclusion criteria were postlingual, moderate to severe sensory neural hearing loss adults; age range 30 to 85 years; word recognition score higher than 72%; no cognitive or neurological deficits. All patients were recruited from Shahreza Rehabilitation Hearing Aid Center affiliated to the Iranian Welfare organization.
Instrumentation
Otoscopic examination, basic audiological tests including Pure Tone Audiometry (PTA), speech audiometry, and acoustic immittance were performed for all participants. PTA was conducted by AC33 (Interacoustic, Denmark). The audiometer and sound field were calibrated based on the American National Standards Institute (ANSI S3.6-2004). The acoustic immittance test (tympanometry and acoustic reflex) was carried out by ZA86 (Pejvak Ava, Iran). The ANL was determined using the Persian version of ANL test. The test is about 20 minutes of a female running story [10]. Also, a 12 talker babble noise was used as the competing noise. Both the running speech and speech babble were presented through a compact disc player routed through the audiometer via a single speaker (Pejvak Ava Ap12 power amplifier, Iran). The speaker was located in front of the patient with 1 meter distance (0° of azimuth). The test was carried out in an anechoic test room. The levels of speech and noise were based on dB HL.
Acceptable noise level procedure
Initially, the patient was trained by oral and written instructions for the 2 following parts of the test. The description was about the goal of experiment, stages of the test, and the task of subject during the test.
Determining the MCL
Patient was instructed and got ready for MCL test with this statement:” You will listen to a story through the loudspeaker that is in your hand. Please pay attention to its loudness carefully and let us know the intensity that is most comfortable for you”. After instruction and ensuring the full understanding of the explanations, the running speech was presented through the speaker. The starting level of speech was 30 dB HL, and according to the patient’s signal, the level was increased or decreased in steps of 5 dB until the most comfortable level was obtained by the patient [9].
Determining the BNL
According to the procedure of MCL, the instruction was also given to the patient. The subject was explained and taught for BNL with this statement: You will listen to the same story with background noise of several individuals talking at the same time. First, the noise level will be turn up until you signal that the noise is too loud for you to understand the story. Then, the noise level will be turn down until you signal that you can understand the story very clearly. Finally, the level of noise will be adjusted to a maximum that you would be willing to “put up with” for a long time while following the story.
After instruction and ensuring full understanding of the explanations, the babble noise was added to the running speech as a competing noise and both were presented to subject. In this step, the starting level of noise was put on 30 dB HL and then, it was increased in the 5 dB steps until a level that the patient could not tolerate. On the final part of the test, the level of noise was adjusted to the 2 dB steps. BNL level was measured for 3 times and the average was recorded as the final level of BNL. Finally, the amount of ANL was calculated using the following formula [11]:
ANL=MCL–BNL
Hearing aid acceptance
In this stage, comprehensive hearing aid counseling was given to the patient. The counseling process included education (awareness, information, inquiry, and consideration), demonstration, discussing options, offering the choices, overcoming objections, and reassurance [12]. The most important part of hearing-aid counseling is the education. Instruction consists of the following 5 levels: Awareness, Information, Inquiry, Consideration, and Statistical methods.
"Awareness" is the first step in counseling education. In this step the patient is notified about what is supposed to be offered to him. In the "information" step the subject is promoted to learn more about how the test can help him.In the "inquiry" level, the curiosity of the subject is incited and he/she starts to ask some questions to learn more about the benefits of hearing aids. In this step of education, the patient spontaneously is involved in the process of working and cooperating with the trainers. "Consideration" can be considered as one of the most significant levels of the current project. In this step, the customer actively ponders taking hearing aid and its services. The other parts of counseling were performed completely, and then, the patient was free to accept or refuse using hearing aid. The decision of the patient was reported as: accepted or refused using hearing aid. In "statistical methods" step, the Kolmogorov–Smirnov (K–S) test was used to assess the normal distribution of data. The Pearson correlation was used to assess the relationships among variables, and the independent t test was used to compare data between groups. All analyses were performed with SPSS version 16 (SPSS Inc. Released 2007. SPSS for Windows, Version 16.0. Chicago, IL, USA).
3. Result
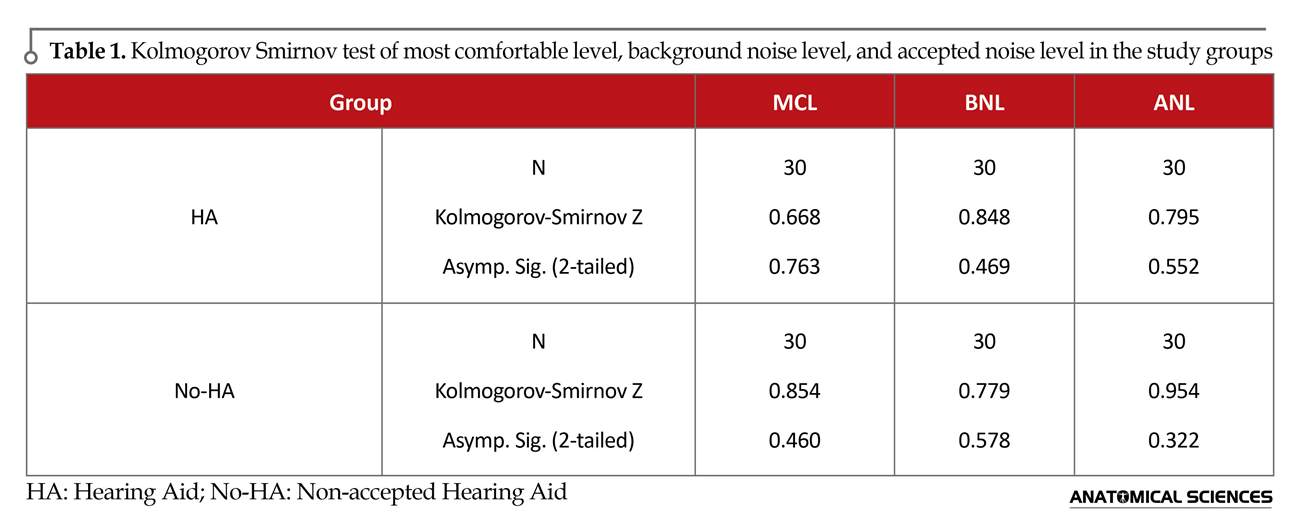
In the present study, a total of 60 participants were assigned to 2 groups: accepted hearing aid (HA) and non-accepted hearing aid (No-HA); subjects’ age range was 30 to 85 years with the mean age of 60 and 63 years in HA and No-HA groups, respectively. There were 20 males and 10 females in HA group and 19 males and 11 females in No-HA group. There was no significant relationship in gender and age between the groups. The mean audiograms showed moderate to severe sensorineural HL. Kolmogorov-Smirnov test for MCL, BNL, and ANL were performed in each group separately (Table 1). There was no significant difference between the groups in each set and the data were normally distributed (Table 1).
Means and Standard Deviations (SD) were averaged across all 30 participants in MCL, BNL, ANL and AGE for both groups and provided in Table 2. The results showed minimum difference between the groups in MCL mean. Similarly, the difference of BNL between two groups was low. ANL mean varied from 7.83±3.08 to 11.73±2.31 among individuals that showed a marked decrease in two groups (Table 2). It was also confirmed by t test between the 2 groups ANL (Table 2). According to the results illustrated in Table 2, there was a significant difference (P≤0.001) between the groups in ANL. The difference was insignificant for MCL (0.813) and BNL (0.07) between the groups.
4. Discussion
The current study aimed at evaluating the acceptable noise level contributes to accept hearing aid in adults with hearing loss. Since there was no association between age and ANL [5], subjects were selected patients within the age range of 30 to 85 years. Also, since gender does not affect ANL [8], the study participants were selected out of both genders. Each participant’s ANL was compared with the acceptance of hearing aid. The results showed that ANL mean in participants who accepted taking hearing aid was lower than the ones who refused to use it.
Hearing loss is beyond a personal problem. It affects patient’s life and can influence his/her relationship with the family, friends, and colleagues [1]. Fortunately, a significant improvement can be achieved in various aspects of life following the diagnosis of hearing loss and the rehabilitation via hearing aid [2, 3]. However, only a few patients with hearing impairments accept using hearing aids. Unfortunately, the usage of hearing aid is not mostly common among the patients with hearing impairments; for example, in the American countries, less than 25% of patients who are candidates for using hearing aids really attempt to use it.
This rate is even lower in the developing countries [4]. It made a group of researchers enthusiastic to study the factors affecting the acceptance and refusal of using hearing aids in such patients. According to the study by Nabelek et al., the main reason is attributed to the problem of amplified ambient noise [5]. In order to answer the question: “How much ambient noise can be bothersome enough to prevent a person from using hearing aid?” they designed and developed a practical speech test called Acceptable Noise Level (ANL) [6].
ANL evaluates the willingness of a listener to hear a continuous speech in the presence of background noise. To perform ANL, first patient’s most comfortable level (MCL) is determined by a speech signal; then, babble noise is added and the patient is asked to adjust it to the highest tolerable level while listening to the speech signal and the story. The obtained level is called the Background Noise Level (BNL). ANL in fact is MCL minus BNL. Practically, ANL is the lowest Signal-to-Noise Ratio (SNR) that a patient can put up with [7]. There is no association between ANL results and gender, hearing sensitivity, age, and speech “perception” in noise [8]. Generally ANL assumption is relied on the fact that some of the patients with hearing impairment do not accept hearing aids, which is the result of their inability to accept the background noise [7].
Since ANL could be a good predictor of this feature, the question is “Who is more successful in the full-time application of hearing aids and who can find it more enjoyable?” and relying on the answers, ANL can be considered as an useful and powerful advisory tool for hearing specialists in all of audiology clinics [6]. According to the realistic expectations, ANL can give audiologists a conception to figure out who needs more advice or who requires more advanced technologies such as directional microphones or assistive listening devices [9]. In other words, what type of patients can tolerate more background noise during a conversation? Briefly, patient’s ANL can give audiologists better and more reliable information to provide more accurate and successful hearing aid counseling.
Although there are many factors for the selection of hearing aid by patient, all of them are subjective and there is no objective measurement tool to assess hearing aid acceptance [9]. Also, the most important factor that influences hearing aid acceptance is patient’s personality and viewpoint in this regard, and according to the results of the current study, there was a significant relationship between the personality and ANL [9]. The main question of the current study was to evaluate the relationship between ANL and hearing aid acceptance in the patients.
Many studies were performed on the relationship between ANL and hearing aid satisfaction, but there was no study on the usage of ANL as the predictor of initial hearing aid acquisition. All studies were focused on the prediction of hearing aid benefits. The current research attempted to improve the rehabilitation given to the patients; authors hope it is useful to other researchers to provide a better understanding the reaction of patients to background noise in order to consider their hearing aid counseling and prescription, and also find out the reason of indifference in some patients with hearing aid acquisition, despite the best efforts the current study maid in hearing aid counseling. The main purpose of the study was to evaluate the relationship between the initial acceptance of hearing aid and individual’s ANL.
2. Materials and Methods
Study subjects
The current study performed on 60 patients with hearing loss who were the candidates for wearing hearing aid; they were assigned to 2 groups: the first group included 30 patients who accepted to take hearing aid and the second group compromised of 30 patients who refused to take hearing aid. The inclusion criteria were postlingual, moderate to severe sensory neural hearing loss adults; age range 30 to 85 years; word recognition score higher than 72%; no cognitive or neurological deficits. All patients were recruited from Shahreza Rehabilitation Hearing Aid Center affiliated to the Iranian Welfare organization.
Instrumentation
Otoscopic examination, basic audiological tests including Pure Tone Audiometry (PTA), speech audiometry, and acoustic immittance were performed for all participants. PTA was conducted by AC33 (Interacoustic, Denmark). The audiometer and sound field were calibrated based on the American National Standards Institute (ANSI S3.6-2004). The acoustic immittance test (tympanometry and acoustic reflex) was carried out by ZA86 (Pejvak Ava, Iran). The ANL was determined using the Persian version of ANL test. The test is about 20 minutes of a female running story [10]. Also, a 12 talker babble noise was used as the competing noise. Both the running speech and speech babble were presented through a compact disc player routed through the audiometer via a single speaker (Pejvak Ava Ap12 power amplifier, Iran). The speaker was located in front of the patient with 1 meter distance (0° of azimuth). The test was carried out in an anechoic test room. The levels of speech and noise were based on dB HL.
Acceptable noise level procedure
Initially, the patient was trained by oral and written instructions for the 2 following parts of the test. The description was about the goal of experiment, stages of the test, and the task of subject during the test.
Determining the MCL
Patient was instructed and got ready for MCL test with this statement:” You will listen to a story through the loudspeaker that is in your hand. Please pay attention to its loudness carefully and let us know the intensity that is most comfortable for you”. After instruction and ensuring the full understanding of the explanations, the running speech was presented through the speaker. The starting level of speech was 30 dB HL, and according to the patient’s signal, the level was increased or decreased in steps of 5 dB until the most comfortable level was obtained by the patient [9].
Determining the BNL
According to the procedure of MCL, the instruction was also given to the patient. The subject was explained and taught for BNL with this statement: You will listen to the same story with background noise of several individuals talking at the same time. First, the noise level will be turn up until you signal that the noise is too loud for you to understand the story. Then, the noise level will be turn down until you signal that you can understand the story very clearly. Finally, the level of noise will be adjusted to a maximum that you would be willing to “put up with” for a long time while following the story.
After instruction and ensuring full understanding of the explanations, the babble noise was added to the running speech as a competing noise and both were presented to subject. In this step, the starting level of noise was put on 30 dB HL and then, it was increased in the 5 dB steps until a level that the patient could not tolerate. On the final part of the test, the level of noise was adjusted to the 2 dB steps. BNL level was measured for 3 times and the average was recorded as the final level of BNL. Finally, the amount of ANL was calculated using the following formula [11]:
ANL=MCL–BNL
Hearing aid acceptance
In this stage, comprehensive hearing aid counseling was given to the patient. The counseling process included education (awareness, information, inquiry, and consideration), demonstration, discussing options, offering the choices, overcoming objections, and reassurance [12]. The most important part of hearing-aid counseling is the education. Instruction consists of the following 5 levels: Awareness, Information, Inquiry, Consideration, and Statistical methods.
"Awareness" is the first step in counseling education. In this step the patient is notified about what is supposed to be offered to him. In the "information" step the subject is promoted to learn more about how the test can help him.In the "inquiry" level, the curiosity of the subject is incited and he/she starts to ask some questions to learn more about the benefits of hearing aids. In this step of education, the patient spontaneously is involved in the process of working and cooperating with the trainers. "Consideration" can be considered as one of the most significant levels of the current project. In this step, the customer actively ponders taking hearing aid and its services. The other parts of counseling were performed completely, and then, the patient was free to accept or refuse using hearing aid. The decision of the patient was reported as: accepted or refused using hearing aid. In "statistical methods" step, the Kolmogorov–Smirnov (K–S) test was used to assess the normal distribution of data. The Pearson correlation was used to assess the relationships among variables, and the independent t test was used to compare data between groups. All analyses were performed with SPSS version 16 (SPSS Inc. Released 2007. SPSS for Windows, Version 16.0. Chicago, IL, USA).
3. Result
In the present study, a total of 60 participants were assigned to 2 groups: accepted hearing aid (HA) and non-accepted hearing aid (No-HA); subjects’ age range was 30 to 85 years with the mean age of 60 and 63 years in HA and No-HA groups, respectively. There were 20 males and 10 females in HA group and 19 males and 11 females in No-HA group. There was no significant relationship in gender and age between the groups. The mean audiograms showed moderate to severe sensorineural HL. Kolmogorov-Smirnov test for MCL, BNL, and ANL were performed in each group separately (Table 1). There was no significant difference between the groups in each set and the data were normally distributed (Table 1).
Means and Standard Deviations (SD) were averaged across all 30 participants in MCL, BNL, ANL and AGE for both groups and provided in Table 2. The results showed minimum difference between the groups in MCL mean. Similarly, the difference of BNL between two groups was low. ANL mean varied from 7.83±3.08 to 11.73±2.31 among individuals that showed a marked decrease in two groups (Table 2). It was also confirmed by t test between the 2 groups ANL (Table 2). According to the results illustrated in Table 2, there was a significant difference (P≤0.001) between the groups in ANL. The difference was insignificant for MCL (0.813) and BNL (0.07) between the groups.
4. Discussion
The current study aimed at evaluating the acceptable noise level contributes to accept hearing aid in adults with hearing loss. Since there was no association between age and ANL [5], subjects were selected patients within the age range of 30 to 85 years. Also, since gender does not affect ANL [8], the study participants were selected out of both genders. Each participant’s ANL was compared with the acceptance of hearing aid. The results showed that ANL mean in participants who accepted taking hearing aid was lower than the ones who refused to use it.
ANL assesses the willingness of a listener to hear a continuous speech in the presence of background noise. ANL test takes about 2 or 3 minutes and its results are reliable and valuable over time even in the listeners with hearing impairment. Nabelek et al., showed that although none of normal hearing listeners (low or high ANLs) had no apparent clinical consequences, patients with hearing impairment who showed high ANLs (≥14 dB) had more problem in use of hearing aid. But, the listeners with hearing impairment and low ANLs (≤8 dB) seem to be comfortable with their amplifications; while, patients with ANL 8 to 14 dB showed different reactions. Harkrider and Tampas suggested that these differences may be attributed to the function of the cochleae and/or auditory nervous systems variations. They also recommended further studies in this regard [13]. Seven years later, Franklin et al., found a relationship between ANL and psychological factors such as the type of personality.
Due to their report, patients who had openness personality had lower ANL and can tolerate more background noise, whereas the ones with conscientious personality had higher ANL and can put up with less background noise [9]. Speech perception in noise scores is not affected by the ANLs and use of hearing aid amplification does not various ANLs. According to this fact, ANL can be used before hearing aid fitting as a predictor. Nebelek et al. found ANL as an accurate objective scale to predict hearing aid satisfaction with 85% validity; they also showed that ANL is a more precise measure rather than SPIN or audiogram type [6].
Although many studies evaluated the relationship between ANL and hearing aid satisfaction, there was no study on the usage of ANL as the predictor for initial hearing aid acquisition. In other words, there was not objective scale in the field of hearing aid acquisition. As ANL is associated with personality [9] and on the other hand, personality is an important factor in the candidacy of hearing aid [14], the current exploratory study was conducted to determine the relationship between the initial acceptance of hearing aid and individual’s ANL. According the results, ANL means in subjects who accepted and refused using hearing aid were 7.83 and 11.73, respectively. Difference between the MCL means in 2 groups was minimal. Similarly, the difference of BNL between the 2 groups was low. In a comparison with Nabelek study, it can be concluded that patients with ANL mean lower than 8 better accepted hearing aids and were the good candidates for hearing aid. Also, patients who had ANL mean higher than 12 refused hearing aid and showed resistance against it.
Since the age did not directly affect hearing aid candidacy and hearing aid acceptance [14], it seems that various age ranges could not be an interfering variable, but for more confirmation and clearness, it needs further investigations. Some of main factors were not considered properly in the current study such as patient cognition, referral center, type of personality, audiologist gender, special conditions of clinic, and patient’s budget. According to these factors, a more controlled research is recommended. In addition, a double-blind research method is also recommended. If the relationship between acceptance of hearing aid and ANL holds true for listeners with hearing loss, then knowing something about a person’s ANL may help audiologists to determine whether the client will most likely be a good candidate for hearing aids.
The current study results showed that lower ANLs are correlated with acceptance of hearing aid and higher ANLs are correlated with resisting against having hearing aid. Participants who accepted taking hearing aid had lower ANL and participants who resisted against taking hearing aid, had higher ANL on average. The current study attempted to improve the rehabilitation given to the patients, and the authors hope it is useful to other researchers to provide a better understanding of how patients react to background noise in order to give hearing aid counseling and prescription, and also find out why some patients are indifferent in hearing aid acquisition, despite the efforts of the current study in offering the best hearing aid counseling.
Acknowledgments
The research was supported by Department of Audiology, School of Rehabilitation, Shahid Beheshti University of Medical Sciences, Tehran, Iran. Authors wish to thank Shahreza Rehabilitation Hearing and Speech Clinic for the cooperation with the study.
Conflict of Interest
The authors declared no conflicts of interest.
References
Due to their report, patients who had openness personality had lower ANL and can tolerate more background noise, whereas the ones with conscientious personality had higher ANL and can put up with less background noise [9]. Speech perception in noise scores is not affected by the ANLs and use of hearing aid amplification does not various ANLs. According to this fact, ANL can be used before hearing aid fitting as a predictor. Nebelek et al. found ANL as an accurate objective scale to predict hearing aid satisfaction with 85% validity; they also showed that ANL is a more precise measure rather than SPIN or audiogram type [6].
Although many studies evaluated the relationship between ANL and hearing aid satisfaction, there was no study on the usage of ANL as the predictor for initial hearing aid acquisition. In other words, there was not objective scale in the field of hearing aid acquisition. As ANL is associated with personality [9] and on the other hand, personality is an important factor in the candidacy of hearing aid [14], the current exploratory study was conducted to determine the relationship between the initial acceptance of hearing aid and individual’s ANL. According the results, ANL means in subjects who accepted and refused using hearing aid were 7.83 and 11.73, respectively. Difference between the MCL means in 2 groups was minimal. Similarly, the difference of BNL between the 2 groups was low. In a comparison with Nabelek study, it can be concluded that patients with ANL mean lower than 8 better accepted hearing aids and were the good candidates for hearing aid. Also, patients who had ANL mean higher than 12 refused hearing aid and showed resistance against it.
Since the age did not directly affect hearing aid candidacy and hearing aid acceptance [14], it seems that various age ranges could not be an interfering variable, but for more confirmation and clearness, it needs further investigations. Some of main factors were not considered properly in the current study such as patient cognition, referral center, type of personality, audiologist gender, special conditions of clinic, and patient’s budget. According to these factors, a more controlled research is recommended. In addition, a double-blind research method is also recommended. If the relationship between acceptance of hearing aid and ANL holds true for listeners with hearing loss, then knowing something about a person’s ANL may help audiologists to determine whether the client will most likely be a good candidate for hearing aids.
The current study results showed that lower ANLs are correlated with acceptance of hearing aid and higher ANLs are correlated with resisting against having hearing aid. Participants who accepted taking hearing aid had lower ANL and participants who resisted against taking hearing aid, had higher ANL on average. The current study attempted to improve the rehabilitation given to the patients, and the authors hope it is useful to other researchers to provide a better understanding of how patients react to background noise in order to give hearing aid counseling and prescription, and also find out why some patients are indifferent in hearing aid acquisition, despite the efforts of the current study in offering the best hearing aid counseling.
Acknowledgments
The research was supported by Department of Audiology, School of Rehabilitation, Shahid Beheshti University of Medical Sciences, Tehran, Iran. Authors wish to thank Shahreza Rehabilitation Hearing and Speech Clinic for the cooperation with the study.
Conflict of Interest
The authors declared no conflicts of interest.
References
- Dalton DS, Cruickshanks KJ, Klein BEK, Klein R, Wiley TL, Nondahl DM. The impact of hearing loss on quality of life in older adults. The Gerontologist. 2003; 43(5):661–8. doi: 10.1093/geront/43.5.661
- Mulrow CD, Tuley MR, Aguilar C. Sustained benefits of hearing aids. Journal of Speech Language and Hearing Research. 1992; 35(6):1402. doi: 10.1044/jshr.3506.1402
- Chisolm TH, Johnson CE, Danhauer JL, Portz LJP, Abrams HB, Lesner S, et al. A systematic review of health related quality of life and hearing aids: Final report of the american academy of audiology task force on the health related quality of life benefits of amplification in adults. Journal of the American Academy of Audiology. 2007; 18(2):151–83. doi: 10.3766/jaaa.18.2.7
- Da Silva DPCB, da Silva VB, Aurélio FS. Auditory satisfaction of patients fitted with hearing aids in the Brazilian Public Health Service and benefits offered by the hearing aids. Brazilian Journal of Otorhinolaryngology. 2013; 79(5):538–45. doi: 10.5935/1808-8694.20130098
- Nabelek AK, Tucker FM, Letowski TR. Toleration of background noises. Journal of Speech Language and Hearing Research. 1991; 34(3):679. doi: 10.1044/jshr.3403.679
- Nabelek AK, Freyaldenhoven MC, Tampas JW, Burchfield SB, Muenchen RA. Acceptable noise level as a predictor of hearing aid use. Journal of the American Academy of Audiology. 2006; 17(9):626–39. doi: 10.3766/jaaa.17.9.2
- Freyaldenhoven MC. Acceptable noise level (ANL): Research and current application. San Antonio: Audiology Online. 2007.
- Rogers DS, Harkrider AW, Burchfield SB, Nabelek AK. The influence of listener's gender on the acceptance of background noise. Journal of the American Academy of Audiology. 2003; 14(7):372-82. PMID: 14620611
- Franklin C, Johnson LV, White L, Franklin C, Smith Olinde L. The relationship between personality type and acceptable noise levels: A pilot study. ISRN Otolaryngology. 2013; 2013:1–6. doi: 10.1155/2013/902532
- Ahmadi A, Fatahi J, Jalilvand H, Jalaie S. [Developing and evaluating the reliability of acceptable noise level test in Persian language (Persian)]. The Scientific Journal of Rehabilitation Medicine. 2015; 4(2):109-17.
- Pourbakht A, Jalilvand H, Jalaee S. The relationship between hearing aid frequency response and acceptable noise level in patients with sensorineural hearing loss. Advanced Biomedical Research. 2015; 4(1):256. doi: 10.4103/2277-9175.170681
- Taylor B. Using scientific principles in the hearing aid consultation [Internet]. 2011 [Updated 2011 September 19]. Availble from: https://www.audiologyonline.com/articles/using-scientific-principles-in-hearing-807
- Harkrider AW, Tampas JW. Differences in responses from the cochleae and central nervous systems of females with low versus high acceptable noise levels. Journal of the American Academy of Audiology. 2006; 17(9):667–76. doi: 10.3766/jaaa.17.9.6
- Dillon H. Hearing aids. New York: Thieme Medical Publishers; 2012.
Type of Study: Original |
Subject:
Gross Anatomy
Received: 2016/09/2 | Accepted: 2017/12/28 | Published: 2018/01/1
Received: 2016/09/2 | Accepted: 2017/12/28 | Published: 2018/01/1
References
1. Dalton DS, Cruickshanks KJ, Klein BEK, Klein R, Wiley TL, Nondahl DM. The impact of hearing loss on quality of life in older adults. The Gerontologist. 2003; 43(5):661–8. doi: 10.1093/geront/43.5.661 [DOI:10.1093/geront/43.5.661]
2. Mulrow CD, Tuley MR, Aguilar C. Sustained benefits of hearing aids. Journal of Speech Language and Hearing Research. 1992; 35(6):1402. doi: 10.1044/jshr.3506.1402 [DOI:10.1044/jshr.3506.1402]
3. Chisolm TH, Johnson CE, Danhauer JL, Portz LJP, Abrams HB, Lesner S, et al. A systematic review of health related quality of life and hearing aids: Final report of the american academy of audiology task force on the health related quality of life benefits of amplification in adults. Journal of the American Academy of Audiology. 2007; 18(2):151–83. doi: 10.3766/jaaa.18.2.7 [DOI:10.3766/jaaa.18.2.7]
4. Da Silva DPCB, da Silva VB, Aurélio FS. Auditory satisfaction of patients fitted with hearing aids in the Brazilian Public Health Service and benefits offered by the hearing aids. Brazilian Journal of Otorhinolaryngology. 2013; 79(5):538–45. doi: 10.5935/1808-8694.20130098 [DOI:10.5935/1808-8694.20130098]
5. Nabelek AK, Tucker FM, Letowski TR. Toleration of background noises. Journal of Speech Language and Hearing Research. 1991; 34(3):679. doi: 10.1044/jshr.3403.679 [DOI:10.1044/jshr.3403.679]
6. Nabelek AK, Freyaldenhoven MC, Tampas JW, Burchfield SB, Muenchen RA. Acceptable noise level as a predictor of hearing aid use. Journal of the American Academy of Audiology. 2006; 17(9):626–39. doi: 10.3766/jaaa.17.9.2 [DOI:10.3766/jaaa.17.9.2]
7. Freyaldenhoven MC. Acceptable noise level (ANL): Research and current application. San Antonio: Audiology Online. 2007. [PMID]
8. Rogers DS, Harkrider AW, Burchfield SB, Nabelek AK. The influence of listener's gender on the acceptance of background noise. Journal of the American Academy of Audiology. 2003; 14(7):372-82. PMID: 14620611 [PMID]
9. Franklin C, Johnson LV, White L, Franklin C, Smith Olinde L. The relationship between personality type and acceptable noise levels: A pilot study. ISRN Otolaryngology. 2013; 2013:1–6. doi: 10.1155/2013/902532 [DOI:10.1155/2013/902532]
10. Ahmadi A, Fatahi J, Jalilvand H, Jalaie S. [Developing and evaluating the reliability of acceptable noise level test in Persian language (Persian)]. The Scientific Journal of Rehabilitation Medicine. 2015; 4(2):109-17.
11. Pourbakht A, Jalilvand H, Jalaee S. The relationship between hearing aid frequency response and acceptable noise level in patients with sensorineural hearing loss. Advanced Biomedical Research. 2015; 4(1):256. doi: 10.4103/2277-9175.170681 [DOI:10.4103/2277-9175.170681]
12. Taylor B. Using scientific principles in the hearing aid consultation [Internet]. 2011 [Updated 2011 September 19]. Availble from: https://www.audiologyonline.com/articles/using-scientific-principles-in-hearing-807
13. Harkrider AW, Tampas JW. Differences in responses from the cochleae and central nervous systems of females with low versus high acceptable noise levels. Journal of the American Academy of Audiology. 2006; 17(9):667–76. doi: 10.3766/jaaa.17.9.6 [DOI:10.3766/jaaa.17.9.6]
14. Dillon H. Hearing aids. New York: Thieme Medical Publishers; 2012.
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
