Sat, Jul 12, 2025
Volume 14, Issue 2 (Summer & Autumn 2017)
ASJ 2017, 14(2): 65-72 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Jalali Kondori B, Asadi M H, Raouf Sarshouri J, Bahadoran H. Optimization of Transient Focal Cerebral Ischemia Model by Middle Cerebral Artery Occlusion. ASJ 2017; 14 (2) :65-72
URL: http://anatomyjournal.ir/article-1-168-en.html
URL: http://anatomyjournal.ir/article-1-168-en.html


1- Department of Anatomical Sciences, School of Medicine, Baqiyatallah University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 504 kb]
(1684 Downloads)
| Abstract (HTML) (4380 Views)




Full-Text: (1918 Views)
1. Introduction
Stroke means a sharp reduction or complete cessation of blood flow in a brain region, preventing needed oxygen and metabolic materials delivery, and removal of waste products from the brain [1]. Stroke can be divided into 2 types: ischemic (artery occlusion) and hemorrhagic (artery rupture). Stroke causes and risk factors are: cerebral thrombosis, cerebral embolism, subarachnoid hemorrhage, and intracerebral hemorrhage. The cerebral thrombosis and cerebral embolism known as ischemic strokes account for 70% to 80% of all cases [2]. Cerebral ischemia is one of the most common causes of death in industrialized communities [3]. The need for animal models is inevitable to study the pathophysiology and treatment of cerebral ischemia in human. The most important features of animal ischemic models are repeatability and similarity to human models [4].
Several approaches can be utilized to create focal cerebral ischemia such as permanent Middle Cerebral Artery Occlusion (MCAO) through craniotomy, embolic MCA occlusion, photothrombosis model, and intra-arterial suture occlusion of MCA [5]. Previous studies showed that high mortality rate of animals in researches, incomplete blockage of the arteries, various degrees of ischemic lesions, and various volumes of cerebral lesions generated in the ischemic area are the disadvantages of these methods [6, 7]. Technical details are also varied among the methods. For example, rat weight or ischemia time is different in methods employed in studies. In general, various techniques with different variables and results indicated the need to introduce a standard procedure in order to create certain focal ischemic lesions. One of the main variables raised in different studies was the weight range of laboratory animals. Given that, the diameter of vessels would be definitely larger by the elevation of body weight; so if heavier rats are used, a specific filament probably does not make the same ischemic volume in rats.
In the present study, the best method was applied to overcome the limitations and variables of MCAO, taking into account the results as well as the advantages and limitations of previous studies in creating focal ischemia. Therefore, by applying the changes, the level of technical success increased as well as a standard and repeatable method was introduced to create focal ischemia in an animal model.
2. Materials and Methods
In the present study, 35 male Wistar rats were divided into 4 groups. The weight of the rats ranged from 250 to 310 g. The animals, before and during the testing, were maintained under standard conditions of 12:12 hours light/dark cycle with proper humidity, temperature of 25°C and free access to food and water. All experiments were performed in accordance with the ethical principles of animal use approved by the Research Council of Baqiyatallah University of Medical Sciences, Tehran, Iran.
The rats were tested in the following groups: 1. Ischemia Group (IG1): Weight range of 250 to 270 g with ischemic induction duration of 60 minutes; 2. Ischemia Group (IG2): Weight range of 250 to 270 g with ischemic induction duration of 90 minutes; 3. Ischemia Group (IG3): Weight range of 250 to 310 g with ischemic induction duration of 60 minutes; 4. Ischemia Group (IG4): Weight range of 250 to 310 g with ischemic induction duration of 90 minutes; and 5. The sham group: All surgical procedures were carried out to establish cerebral ischemia, but filament placement and ischemic induction not performed in this group.
Cerebral focal ischemic induction
For cerebral transient focal ischemic induction, MCA was blocked by MCAO, as follows: The rats anesthetized by 4% isoflurane were placed in supine position and their shaved neck area was cleaned and disinfected. The 2.5% isoflurane was used to induce anesthesia. A longitudinal incision was performed in the midline of the anterior part of the neck. After removing the skin, salivary glands, muscles on the right side of the sectioned area, common carotid artery, external carotid, and internal carotid right were observed. The vagus nerve and carotid body were carefully separated from them. Connective tissue and adjacent elements of the internal carotid artery were pushed until the origin of this branch to prevent the entry of filaments into pterygopalatine artery. The pterygopalatine artery was temporarily blocked using surgical thread.
Occipital artery and superior thyroid artery, the branches of the external carotid artery, were carefully blocked. Then, the black braided nylon, 0-3 gauge (ethicon) with rounded head through the heat was directed into the internal carotid artery via external carotid artery to deal with the resistance and block the middle cerebral artery. After creating ischemia, the filament was removed and reperfusion was established for 24 hours. During the surgery, rectal temperature was measured by a digital thermometer and maintained at about 37°C using heat lamps and pads.
Assessment of neuromotor dysfunction
Animals 24 hours after creating the ischemia were evaluated for the incidence of Neurological Deficit Score (NDS) caused by ischemia. A specific test introduced by Pelseniyla et al. was used to this end. In this test, score 1 was given to rats with natural motion; score 2 to the animal that bended the front leg on the opposite side of the lesion or reduced the ability of gripping in that organs while hangs down from the tail; score 3 to the animal that began to turn toward the ischemic hemisphere (left) at the start of motion on a flat surface, which was at normal state at the rest time; score 4 to the animal that had lost righting reflex or had little resistance against the righting by pushing to lateral positions; score 5 to the animal with no spontaneity motion.
Measurement of brain lesion volume
After evaluation of neuromotor dysfunction, the animals were anesthetized by ether. The brain was removed after creating cervical dislocation. Then, 2-mm coronal sections were prepared using brain matrix. For staining, the samples were placed in 2% Triphenyl-Tetrazolium Chloride (TTC) solution at 37°C for 20 minutes. The ischemic areas appeared in white and healthy areas in red. The sections were placed in 10% buffered formalin to be fixed for 24 hours.
After final preparation, the images of sections were taken separately through a digital camera (Cannon, Japan). The surface area of the damaged parts of the cortex and striatum was measured for each section using the NIH image analyzer software. The lesion volume was calculated as a percentage of total volume for all sections.
Histopathologic studies
To evaluate the histopathological changes, 5-micron sections were prepared from tissue samples. Cresyl violet acetate staining was utilized to evaluate the morphology of cells and changes following ischemia.
Statistical analysis
The obtained results were expressed as mean±Standard Error of Mean (SEM). The Student t test was used for intergroup comparison and P<0.05 was considered as level of significance.
3. Results
No motor dysfunction was observed in the control group 24 hours after ischemia (NDS=1), but neuromotor dysfunctions were found in other ischemic groups and neurologic test scores were higher in the intervention groups, compared to the controls. Assessment of neuromotor dysfunctions among the ischemic groups showed that NDS was higher in groups with 90-minute ischemic durations compared with the ones with 60 minutes duration. Between the 2 groups with 60-minute ischemic duration, the NDS score was higher in the animals with lower weights. As seen in Figure 1, the NDS score distribution among the groups with higher weights was more than the lower weight ones. The mortality rate in the groups 1, 2, 3 and 4 was 3.6%, 5.2%, 5.5% and 9%, respectively.
Stroke means a sharp reduction or complete cessation of blood flow in a brain region, preventing needed oxygen and metabolic materials delivery, and removal of waste products from the brain [1]. Stroke can be divided into 2 types: ischemic (artery occlusion) and hemorrhagic (artery rupture). Stroke causes and risk factors are: cerebral thrombosis, cerebral embolism, subarachnoid hemorrhage, and intracerebral hemorrhage. The cerebral thrombosis and cerebral embolism known as ischemic strokes account for 70% to 80% of all cases [2]. Cerebral ischemia is one of the most common causes of death in industrialized communities [3]. The need for animal models is inevitable to study the pathophysiology and treatment of cerebral ischemia in human. The most important features of animal ischemic models are repeatability and similarity to human models [4].
Several approaches can be utilized to create focal cerebral ischemia such as permanent Middle Cerebral Artery Occlusion (MCAO) through craniotomy, embolic MCA occlusion, photothrombosis model, and intra-arterial suture occlusion of MCA [5]. Previous studies showed that high mortality rate of animals in researches, incomplete blockage of the arteries, various degrees of ischemic lesions, and various volumes of cerebral lesions generated in the ischemic area are the disadvantages of these methods [6, 7]. Technical details are also varied among the methods. For example, rat weight or ischemia time is different in methods employed in studies. In general, various techniques with different variables and results indicated the need to introduce a standard procedure in order to create certain focal ischemic lesions. One of the main variables raised in different studies was the weight range of laboratory animals. Given that, the diameter of vessels would be definitely larger by the elevation of body weight; so if heavier rats are used, a specific filament probably does not make the same ischemic volume in rats.
In the present study, the best method was applied to overcome the limitations and variables of MCAO, taking into account the results as well as the advantages and limitations of previous studies in creating focal ischemia. Therefore, by applying the changes, the level of technical success increased as well as a standard and repeatable method was introduced to create focal ischemia in an animal model.
2. Materials and Methods
In the present study, 35 male Wistar rats were divided into 4 groups. The weight of the rats ranged from 250 to 310 g. The animals, before and during the testing, were maintained under standard conditions of 12:12 hours light/dark cycle with proper humidity, temperature of 25°C and free access to food and water. All experiments were performed in accordance with the ethical principles of animal use approved by the Research Council of Baqiyatallah University of Medical Sciences, Tehran, Iran.
The rats were tested in the following groups: 1. Ischemia Group (IG1): Weight range of 250 to 270 g with ischemic induction duration of 60 minutes; 2. Ischemia Group (IG2): Weight range of 250 to 270 g with ischemic induction duration of 90 minutes; 3. Ischemia Group (IG3): Weight range of 250 to 310 g with ischemic induction duration of 60 minutes; 4. Ischemia Group (IG4): Weight range of 250 to 310 g with ischemic induction duration of 90 minutes; and 5. The sham group: All surgical procedures were carried out to establish cerebral ischemia, but filament placement and ischemic induction not performed in this group.
Cerebral focal ischemic induction
For cerebral transient focal ischemic induction, MCA was blocked by MCAO, as follows: The rats anesthetized by 4% isoflurane were placed in supine position and their shaved neck area was cleaned and disinfected. The 2.5% isoflurane was used to induce anesthesia. A longitudinal incision was performed in the midline of the anterior part of the neck. After removing the skin, salivary glands, muscles on the right side of the sectioned area, common carotid artery, external carotid, and internal carotid right were observed. The vagus nerve and carotid body were carefully separated from them. Connective tissue and adjacent elements of the internal carotid artery were pushed until the origin of this branch to prevent the entry of filaments into pterygopalatine artery. The pterygopalatine artery was temporarily blocked using surgical thread.
Occipital artery and superior thyroid artery, the branches of the external carotid artery, were carefully blocked. Then, the black braided nylon, 0-3 gauge (ethicon) with rounded head through the heat was directed into the internal carotid artery via external carotid artery to deal with the resistance and block the middle cerebral artery. After creating ischemia, the filament was removed and reperfusion was established for 24 hours. During the surgery, rectal temperature was measured by a digital thermometer and maintained at about 37°C using heat lamps and pads.
Assessment of neuromotor dysfunction
Animals 24 hours after creating the ischemia were evaluated for the incidence of Neurological Deficit Score (NDS) caused by ischemia. A specific test introduced by Pelseniyla et al. was used to this end. In this test, score 1 was given to rats with natural motion; score 2 to the animal that bended the front leg on the opposite side of the lesion or reduced the ability of gripping in that organs while hangs down from the tail; score 3 to the animal that began to turn toward the ischemic hemisphere (left) at the start of motion on a flat surface, which was at normal state at the rest time; score 4 to the animal that had lost righting reflex or had little resistance against the righting by pushing to lateral positions; score 5 to the animal with no spontaneity motion.
Measurement of brain lesion volume
After evaluation of neuromotor dysfunction, the animals were anesthetized by ether. The brain was removed after creating cervical dislocation. Then, 2-mm coronal sections were prepared using brain matrix. For staining, the samples were placed in 2% Triphenyl-Tetrazolium Chloride (TTC) solution at 37°C for 20 minutes. The ischemic areas appeared in white and healthy areas in red. The sections were placed in 10% buffered formalin to be fixed for 24 hours.
After final preparation, the images of sections were taken separately through a digital camera (Cannon, Japan). The surface area of the damaged parts of the cortex and striatum was measured for each section using the NIH image analyzer software. The lesion volume was calculated as a percentage of total volume for all sections.
Histopathologic studies
To evaluate the histopathological changes, 5-micron sections were prepared from tissue samples. Cresyl violet acetate staining was utilized to evaluate the morphology of cells and changes following ischemia.
Statistical analysis
The obtained results were expressed as mean±Standard Error of Mean (SEM). The Student t test was used for intergroup comparison and P<0.05 was considered as level of significance.
3. Results
No motor dysfunction was observed in the control group 24 hours after ischemia (NDS=1), but neuromotor dysfunctions were found in other ischemic groups and neurologic test scores were higher in the intervention groups, compared to the controls. Assessment of neuromotor dysfunctions among the ischemic groups showed that NDS was higher in groups with 90-minute ischemic durations compared with the ones with 60 minutes duration. Between the 2 groups with 60-minute ischemic duration, the NDS score was higher in the animals with lower weights. As seen in Figure 1, the NDS score distribution among the groups with higher weights was more than the lower weight ones. The mortality rate in the groups 1, 2, 3 and 4 was 3.6%, 5.2%, 5.5% and 9%, respectively.
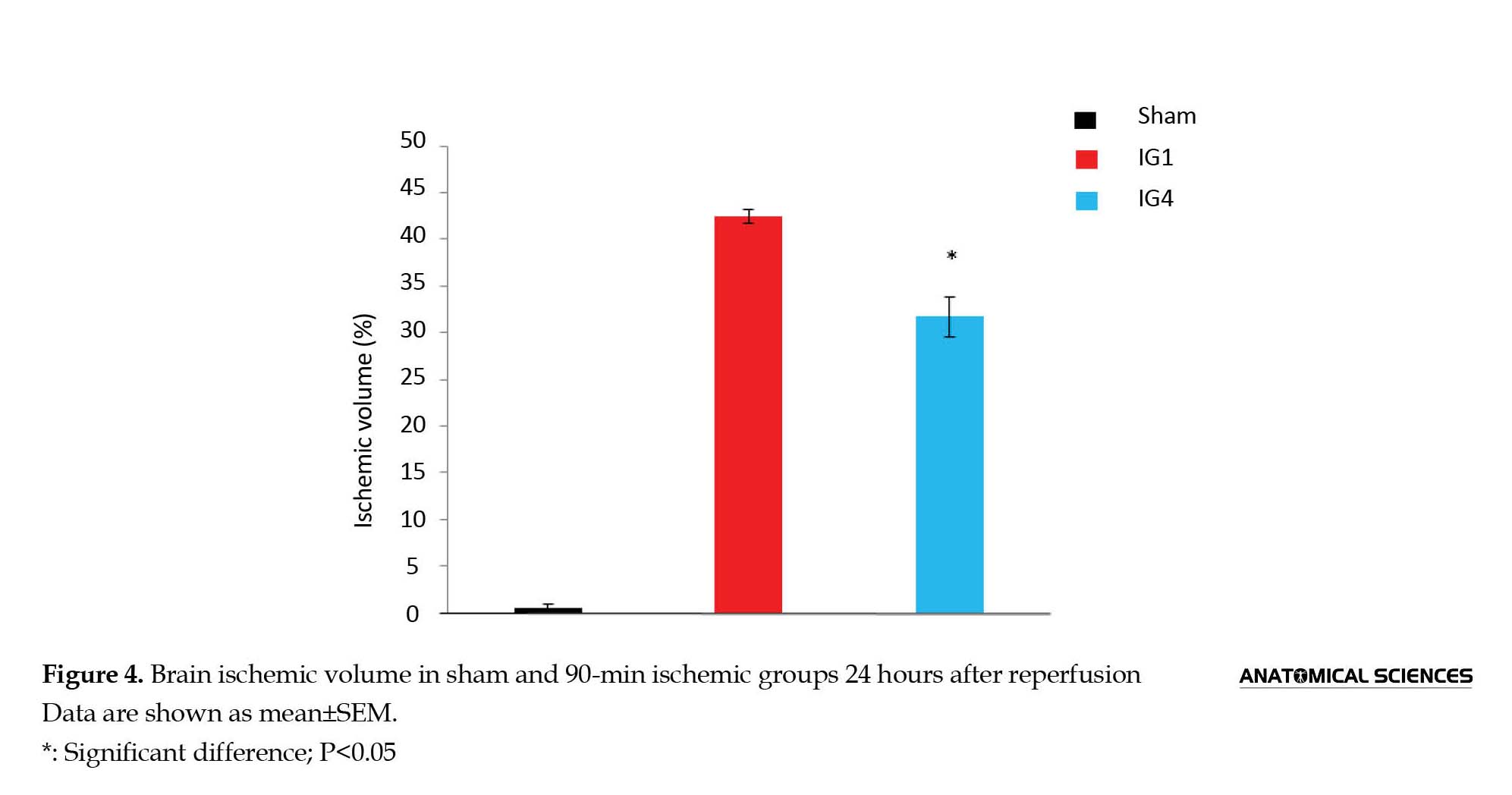
Results of the current study also indicated that the ischemic lesion volume in group 2 was higher than other groups (Figure 2). The ischemic areas are shown in white and the non-ischemic areas in red. As shown in Figure 3, the ischemic lesion volume in 60-minute ischemic groups was significantly higher in the animals with lower weights; the same results were obtained for 90-minute ischemic groups (Figure 4). The results also showed that the lesion volume among the groups with higher weight had more changes.
In histopathological studies, the Nissl bodies were stained using cresyl violet acetate solution. As seen in Figure 5, no pathological changes were observed in the control group. In ischemic groups, neurons had dense and shrunken nuclei. The numbers of cells in the IG1, IG2, and IG3 groups were fallen sharply compared with the control group and neurons with dense nuclei were visible. The cell damage rate was less in the group IG4 and healthy neurons were obvious alongside the damaged and dense neurons.
4. Discussion
The high prevalence of stroke disease in the industrialized countries indicated the need for efforts to identify risk factors and methods to treat the disease. The use of similar animal models to simulate cerebral ischemia and evaluate the therapeutic strategies can be very beneficial. Extensive clinical studies on stroke in humans indicated that the infarct size in ischemic stroke was very small and limited in most cases. A human clinical trial showed that brain infarct size often ranges from 28 to 80 cubic millimeters [8]. Another clinical research revealed that malignant infarction in human ischemia is observed only in 10% of the cases [9]. The most advantageous point in the advanced animal models is their similarity to the human models; hence, the use of methods to create permanent ischemia does not seem desirable. In addition to this advantage, high mortality rate, complicated surgical procedures, and extensive changes in the size and location of brain lesions limited the application of such models in cerebral ischemia studies.
In subsequent studies, the transient MCAO by intra-arterial filament placement method were used; one of the advantages of this method is the reversibility of artery occlusion. In addition, the transient MCAO is a convenient technique with shorter surgical time and lower cost. This technique was gradually changed. For example, the heating and forming the filament tip technique was used to better blockage in the artery [10, 11]. The filament tip covered by silicone and polymers is a technique applied in recent studies. Although the use of silicon in forming filaments increased the efficiency of ischemic lesions, some researchers believe that the separation of the silicon particles can lead to the incidence of vascular occlusion. Ethicon 0-3 filament was used in the current study. The filament tip was formed using heat in a particular way. The shaped form was studied carefully under a light microscope to ensure regular and uniform shape.
The results obtained from the method of intra-arterial filament placement for focal ischemia in animal models are very different because of various variables and variation in details. In the current study, different variables were evaluated in order to introduce a standard and repeatable approach for inducing transient focal ischemia. The variables of previous studies were the ischemic duration, weight of the rats, anesthetics, etc. The researchers utilized the periods of 60, 90 and 120 minute in the intra-arterial filament placement method. Garcia and Li demonstrated that the periods longer than 60 minutes could lead to create larger ischemia, especially in the hippocampal and hypothalamic areas [12]. Damage to cells in hypothalamus caused hyperthermia in rats within the 24 hours after ischemia [13]. The incidence of hyperthermia resulted in increased cell death and animal mortality [14]. In addition, studies suggest that damage to the hypothalamus was rarely observed in human ischemic. Animal models should be designed in such an extent to do not damage the vast area of hypothalamus.
It is also important to note that striatal damages begin in a short interval of ischemia and generally cause necrosis in cells, but cortical damages start with delay and gradually result in cell apoptosis [15]. Therefore, reperfusion reduces cell damage in the cortex. Moreover, hypoxia-induced genes such as heat shock protein 70, Bcl-2, Bcl- XL, and Bax with neuroprotective role can exclusively be expressed in the cortex [16, 17].
Animal model that in addition to the limited damage to ischemic core area can cause a delayed death in the cortex has acceptable similarity to human ischemia [18]. According to these reasons, the 60-minute ischemic duration is more appropriate for creating ischemia similar to humans in animal models. Results of the current study also confirmed this issue. In histopathological assessments of cerebral ischemic samples, the pathological changes were reported including the formation of eosinophilic neurons (neurons with pyknotic, shrieked, dense, and triangular nuclei with highly acidophilic cytoplasm).
In the current study, the histopathological changes were clearly observed in the ischemic groups. Another variable in intra-arterial filament placement method was the weight rage of rats. Given that, the diameter of vessels would be larger definitely by increasing the body weight, so if heavier rats are used in a group, a specific filament probably does not give the same ischemic volume in rats. For example, Oliff et al., studied rats weighed 276 to 346 g. The success rate of intra-arterial filament placement method was 70% in their study; a lower efficiency compared with the studies on rats with lower weights was observed [19, 20]. The results of the current study clearly showed that using smaller rats increased the accuracy and repeatability of intra-arterial filament placement method and reduced mortality.
The method of inducing anesthesia in rats was another variable considered in other studies. Some studies used a combination of ketamine and xylazine for animal anesthesia that the mortality rate of the method was very high due to respiratory and cardiovascular disorders alongside of a long recovery time. The use of isoflurane in animal anesthesia caused a significant reduction in mortality and recovery time. Moreover, studies show that isoflurane has neuroprotective effects on rats’ recovery [21]. The focal ischemia model was developed in rats and mice. Hypothalamic ischemia caused hypothermia in mice unlike rats, and required intensive care during the recovery period [22]. Also, unlike rats, the damage levels caused by ischemia varied in different murine races. For example, the damage levels caused by ischemia were higher in BALB/c mice than that of C57BL/6 mice [23].
In different races of mice, collateral arteries had various patterns. In addition, the sensitivity level of cells to ischemia varied in different races of mice. In the murine model, ischemic lesion volume was directly related to the artery occlusion and followed it dramatically. For example, ischemic lesion volume caused by artery occlusion in C57BL/6 mice for 30 minutes was about 5 times higher than the occlusion for 15 minutes [24], or bilateral common carotid artery occlusion for 3 minutes did not create visible ischemic lesion, whereas obstruction for 5 minutes caused ischemic lesion in the hypothalamus and the striatum. Considering these characteristics, using rats in order to create optimal models of focal ischemia seems more reasonable.
The present study aimed at making a comprehensive review of previous studies on creating animal models of focal cerebral ischemia in order to introduce a standard method with high repeatability and efficiency. Based on the results of the current study, it is suggested to use rats with lower weights for creating animal ischemia model that can be generalized to ischemia in humans. The use of isoflurane for animal anesthesia was more appropriate compared with other anesthetic agents. In addition, results of the study suggested that it is better to create transient focal ischemia model by MCAO using Ethicon thread formed for 60 minutes.
Acknowledgements
This research did not receive any specific grant from funding agencies in the public, commercial, or not-forprofit sectors. We would like to thank Dr. Mohamad Hossein Asadi, head of Department of Anatomical Sciences, Baqiyatallah University of Medical Sciences, for his guidance and support in this study.
Conflict of Interest
The authors declared no conflicts of interest.
References
The high prevalence of stroke disease in the industrialized countries indicated the need for efforts to identify risk factors and methods to treat the disease. The use of similar animal models to simulate cerebral ischemia and evaluate the therapeutic strategies can be very beneficial. Extensive clinical studies on stroke in humans indicated that the infarct size in ischemic stroke was very small and limited in most cases. A human clinical trial showed that brain infarct size often ranges from 28 to 80 cubic millimeters [8]. Another clinical research revealed that malignant infarction in human ischemia is observed only in 10% of the cases [9]. The most advantageous point in the advanced animal models is their similarity to the human models; hence, the use of methods to create permanent ischemia does not seem desirable. In addition to this advantage, high mortality rate, complicated surgical procedures, and extensive changes in the size and location of brain lesions limited the application of such models in cerebral ischemia studies.
In subsequent studies, the transient MCAO by intra-arterial filament placement method were used; one of the advantages of this method is the reversibility of artery occlusion. In addition, the transient MCAO is a convenient technique with shorter surgical time and lower cost. This technique was gradually changed. For example, the heating and forming the filament tip technique was used to better blockage in the artery [10, 11]. The filament tip covered by silicone and polymers is a technique applied in recent studies. Although the use of silicon in forming filaments increased the efficiency of ischemic lesions, some researchers believe that the separation of the silicon particles can lead to the incidence of vascular occlusion. Ethicon 0-3 filament was used in the current study. The filament tip was formed using heat in a particular way. The shaped form was studied carefully under a light microscope to ensure regular and uniform shape.
The results obtained from the method of intra-arterial filament placement for focal ischemia in animal models are very different because of various variables and variation in details. In the current study, different variables were evaluated in order to introduce a standard and repeatable approach for inducing transient focal ischemia. The variables of previous studies were the ischemic duration, weight of the rats, anesthetics, etc. The researchers utilized the periods of 60, 90 and 120 minute in the intra-arterial filament placement method. Garcia and Li demonstrated that the periods longer than 60 minutes could lead to create larger ischemia, especially in the hippocampal and hypothalamic areas [12]. Damage to cells in hypothalamus caused hyperthermia in rats within the 24 hours after ischemia [13]. The incidence of hyperthermia resulted in increased cell death and animal mortality [14]. In addition, studies suggest that damage to the hypothalamus was rarely observed in human ischemic. Animal models should be designed in such an extent to do not damage the vast area of hypothalamus.
It is also important to note that striatal damages begin in a short interval of ischemia and generally cause necrosis in cells, but cortical damages start with delay and gradually result in cell apoptosis [15]. Therefore, reperfusion reduces cell damage in the cortex. Moreover, hypoxia-induced genes such as heat shock protein 70, Bcl-2, Bcl- XL, and Bax with neuroprotective role can exclusively be expressed in the cortex [16, 17].
Animal model that in addition to the limited damage to ischemic core area can cause a delayed death in the cortex has acceptable similarity to human ischemia [18]. According to these reasons, the 60-minute ischemic duration is more appropriate for creating ischemia similar to humans in animal models. Results of the current study also confirmed this issue. In histopathological assessments of cerebral ischemic samples, the pathological changes were reported including the formation of eosinophilic neurons (neurons with pyknotic, shrieked, dense, and triangular nuclei with highly acidophilic cytoplasm).
In the current study, the histopathological changes were clearly observed in the ischemic groups. Another variable in intra-arterial filament placement method was the weight rage of rats. Given that, the diameter of vessels would be larger definitely by increasing the body weight, so if heavier rats are used in a group, a specific filament probably does not give the same ischemic volume in rats. For example, Oliff et al., studied rats weighed 276 to 346 g. The success rate of intra-arterial filament placement method was 70% in their study; a lower efficiency compared with the studies on rats with lower weights was observed [19, 20]. The results of the current study clearly showed that using smaller rats increased the accuracy and repeatability of intra-arterial filament placement method and reduced mortality.
The method of inducing anesthesia in rats was another variable considered in other studies. Some studies used a combination of ketamine and xylazine for animal anesthesia that the mortality rate of the method was very high due to respiratory and cardiovascular disorders alongside of a long recovery time. The use of isoflurane in animal anesthesia caused a significant reduction in mortality and recovery time. Moreover, studies show that isoflurane has neuroprotective effects on rats’ recovery [21]. The focal ischemia model was developed in rats and mice. Hypothalamic ischemia caused hypothermia in mice unlike rats, and required intensive care during the recovery period [22]. Also, unlike rats, the damage levels caused by ischemia varied in different murine races. For example, the damage levels caused by ischemia were higher in BALB/c mice than that of C57BL/6 mice [23].
In different races of mice, collateral arteries had various patterns. In addition, the sensitivity level of cells to ischemia varied in different races of mice. In the murine model, ischemic lesion volume was directly related to the artery occlusion and followed it dramatically. For example, ischemic lesion volume caused by artery occlusion in C57BL/6 mice for 30 minutes was about 5 times higher than the occlusion for 15 minutes [24], or bilateral common carotid artery occlusion for 3 minutes did not create visible ischemic lesion, whereas obstruction for 5 minutes caused ischemic lesion in the hypothalamus and the striatum. Considering these characteristics, using rats in order to create optimal models of focal ischemia seems more reasonable.
The present study aimed at making a comprehensive review of previous studies on creating animal models of focal cerebral ischemia in order to introduce a standard method with high repeatability and efficiency. Based on the results of the current study, it is suggested to use rats with lower weights for creating animal ischemia model that can be generalized to ischemia in humans. The use of isoflurane for animal anesthesia was more appropriate compared with other anesthetic agents. In addition, results of the study suggested that it is better to create transient focal ischemia model by MCAO using Ethicon thread formed for 60 minutes.
Acknowledgements
This research did not receive any specific grant from funding agencies in the public, commercial, or not-forprofit sectors. We would like to thank Dr. Mohamad Hossein Asadi, head of Department of Anatomical Sciences, Baqiyatallah University of Medical Sciences, for his guidance and support in this study.
Conflict of Interest
The authors declared no conflicts of interest.
References
- Dirnagl U, Iadecola C, Moskowitz MA. Pathobiology of ischaemic stroke: An integrated view. Trends in Neurosciences. 1999; 22(9):391-7. doi: 10.1016/s0166-2236(99)01401-0
- Ustrell X, Pellisé A. Cardiac workup of ischemic stroke. Current Cardiology Reviews. 2010; 6(3):175-83. doi: 10.2174/157340310791658721
- Sacco RL, Adams R, Albers G, Alberts MJ, Benavente O, Furie K, et al. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: A statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke. Stroke. 2006; 37(2):577-617. doi: 10.1161/01.str.0000199147.30016.74
- de Leciñana MA, Díez Tejedor E, Carceller F, Roda JM. Cerebral ischemia: From animal studies to clinical practice; Should the methods be reviewed. Cerebrovascular Diseases. 2001; 11(Suppl. 1):20-30. doi: 10.1159/000049122
- Carmichael ST. Rodent models of focal stroke: Size, mechanism, and purpose. NeuroRx. 2005; 2(3):396-409. doi: 10.1602/neurorx.2.3.396
- Beech JS, Williams SC, Campbell CA, Bath PM, Parsons AA, Hunter AJ, Menon DK. Further characterisation of a thromboembolic model of stroke in the rat. Brain Research. 2001; 895(1-2):18-24. doi: 10.1016/s0006-8993(00)03331-x
- Panahpour H. [Role of angiotensin–converting enzyme and AT1 receptor in brain injury, edema and blood brain barrier disruption following transient focal cerebral ischemia in rat (Persian)] [PhD dissertation]. Shiraz: Shiraz University of Medical Sciences; 2008.
- Gladstone DJ. Toward wisdom from failure: Lessons from neuroprotective stroke trials and new therapeutic directions. Stroke. 2002; 33(8):2123-36. doi: 10.1161/01.str.0000025518.34157.51
- Hacke W, Schwab S, Horn M, Spranger M, De Georgia M, Von Kummer R. 'Malignant'middle cerebral artery territory infarction: Clinical course and prognostic signs. Archives of Neurology. 1996; 53(4):309-15. doi: 10.1001/archneur.1996.00550040037012
- Koizumi JY. Experimental studies of ischemic brain edema: 1. New experimental model of cerebral embolism in rats in which recirculation can be introduced in the ischemic area. Japanese Journal of Stroke. 1986; 8(1):1-8. doi: 10.3995/jstroke.8.1
- Longa EZ, Weinstein PR, Carlson S, Cummins R. Reversible middle cerebral artery occlusion without craniectomy in rats. Stroke. 1989; 20(1):84-91. doi: 10.1161/01.str.20.1.84
- Garcia JH, Liu KF, Ho KL. Neuronal necrosis after middle cerebral artery occlusion in Wistar rats progresses at different time intervals in the caudoputamen and the cortex. Stroke. 1995; 26(4):636-43. doi: 10.1161/01.str.26.4.636
- Dietrich WD, Kuluz JW. Spontaneous hyperthermia and its mechanism in the intraluminal suture middle cerebral artery occlusion model of the rat. Stroke. 1999; 30(11):2470-1. doi: 10.1161/01.str.30.11.2464
- Reglodi D, Somogyvari Vigh A, Maderdrut JL, Vigh S, Arimura A. Postischemic spontaneous hyperthermia and its effects in middle cerebral artery occlusion in the rat. Experimental Neurology. 2000; 163(2):399-407. doi: 10.1006/exnr.2000.7367
- Takagi K, Zhao W, Busto R, Ginsberg MD. Local hemodynamic changes during transient middle cerebral artery occlusion and recirculation in the rat: A [14 C] iodoantipyrine autoradiographic study. Brain Research. 1995; 691(1-2):160-8. doi: 10.1016/0006-8993(95)00657-c
- Yokota C, Kaji T, Kuge Y, Inoue H, Tamaki N, Minematsu K. Temporal and topographic profiles of cyclooxygenase-2 expression during 24 h of focal brain ischemia in rats. Neuroscience Letters. 2004; 357(3):219-22. doi: 10.1016/j.neulet.2003.12.109
- Zhu DY, Deng Q, Yao HH, Wang DC, Deng Y, Liu GQ. Inducible nitric oxide synthase expression in the ischemic core and penumbra after transient focal cerebral ischemia in mice. Life Sciences. 2002; 71(17):1985-96. doi: 10.1016/s0024-3205(02)01970-7
- Cheng YD, Al Khoury L, Zivin JA. Neuroprotection for ischemic stroke: Two decades of success and failure. NeuroRx. 2004; 1(1):36-45. doi: 10.1602/neurorx.1.1.36
- Kuge Y, Minematsu K, Yamaguchi T, Miyake Y. Nylon monofilament for intraluminal middle cerebral artery occlusion in rats. Stroke. 1995; 26(9):1655-8. doi: 10.1161/01.str.26.9.1655
- Oliff HS, Weber E, Eilon G, Marek P. The role of strain/vendor differences on the outcome of focal ischemia induced by intraluminal middle cerebral artery occlusion in the rat. Brain Research. 1995; 675(1-2):20-6. doi: 10.1016/0006-8993(95)00033-m
- Sakai H, Sheng H, Yates RB, Ishida K, Pearlstein RD, Warner DS. Isoflurane provides long-term protection against focal cerebral ischemia in the rat. Anesthesiology: The Journal of the American Society of Anesthesiologists. 2007; 106(1):92-9. doi: 10.1097/00000542-200701000-00017
- Barber PA, Hoyte L, Colbourne F, Buchan AM. Temperature-regulated model of focal ischemia in the mouse. Stroke. 2004; 35(7):1720-5. doi: 10.1161/01.str.0000129653.22241.d7
- Lambertsen KL, Gregersen R, Finsen B. Microglial macrophage synthesis of tumor necrosis factor after focal cerebral ischemia in mice is strain dependent. Journal of Cerebral Blood Flow & Metabolism. 2002; 22(7):785-97. doi: 10.1097/00004647-200207000-00004
- McColl BW, Carswell HV, McCulloch J, Horsburgh K. Extension of cerebral hypoperfusion and ischaemic pathology beyond MCA territory after intraluminal filament occlusion in C57Bl/6J mice. Brain Research. 2004; 997(1):15-23. doi: 10.1016/j.brainres.2003.10.028
Type of Study: Original |
Received: 2016/12/12 | Accepted: 2017/03/15 | Published: 2017/07/1
Received: 2016/12/12 | Accepted: 2017/03/15 | Published: 2017/07/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
