Tue, Jul 14, 2026
Volume 20, Issue 2 (Summer & Autumn 2023)
ASJ 2023, 20(2): 63-66 |
Back to browse issues page



![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
G P. Sternal Foramen: A Common Anatomical Variation With Clinical Relevance to Vital Thoracic Structures. ASJ 2023; 20 (2) :63-66
URL: http://anatomyjournal.ir/article-1-599-en.html
URL: http://anatomyjournal.ir/article-1-599-en.html



Panimalar Medical College, Hospital & Research Institute, Chennai, India.
Keywords: Manubrium sterni, Body of sternum, Xiphoid process, Sternal foramen, Sternebrae, Perforated sternum.
Full-Text [PDF 791 kb]
(567 Downloads)
| Abstract (HTML) (2968 Views)
Full-Text: (467 Views)
Introduction
The sternal foramen results from incomplete fusion of the cartilaginous neonatal sternum and is typically found in the lower third of the sternal body. The average diameter of the foramen is 6.5 mm. This anatomical variation was first described by Eustachius in 1707 [1].
The sternum develops from the fusion of two cartilaginous plates along the mid-ventral line. It consists of three components: The manubrium, body, and xiphoid process. Ossification centers for the manubrium and first and second sternebrae appear in the 5th month of fetal life, while those for the third and fourth sternebrae typically appear in the fifth and sixth months, respectively. Fusion of the sternebrae begins at puberty and completes around the 25th year of life. A sternal foramen may occur between the third and fourth sternebrae due to ossification defects. Although often clinically insignificant, its presence must be considered during sternal interventions due to the underlying vital structures [2-4].
Patients with a sternal foramen are generally asymptomatic, often discovering the anomaly incidentally through radiological imaging or midline sternotomy. Awareness of the occurrence of sternal foramen is crucial for radiologists and surgeons. This study investigates the prevalence and anatomical characteristics of the sternal foramen.
Materials and Methods
A descriptive study was conducted on 100 adult sternums collected from the Department of Anatomy, Panimalar Medical College, Hospital, and Research Institute, Tamil Nadu, between April 2021 and April 2022. The presence of a fully formed sternal foramen was assessed visually by two independent investigators. Damaged or abnormally shaped sternums were excluded from the study.
The foramen was measured using a vernier caliper (Figure 1).

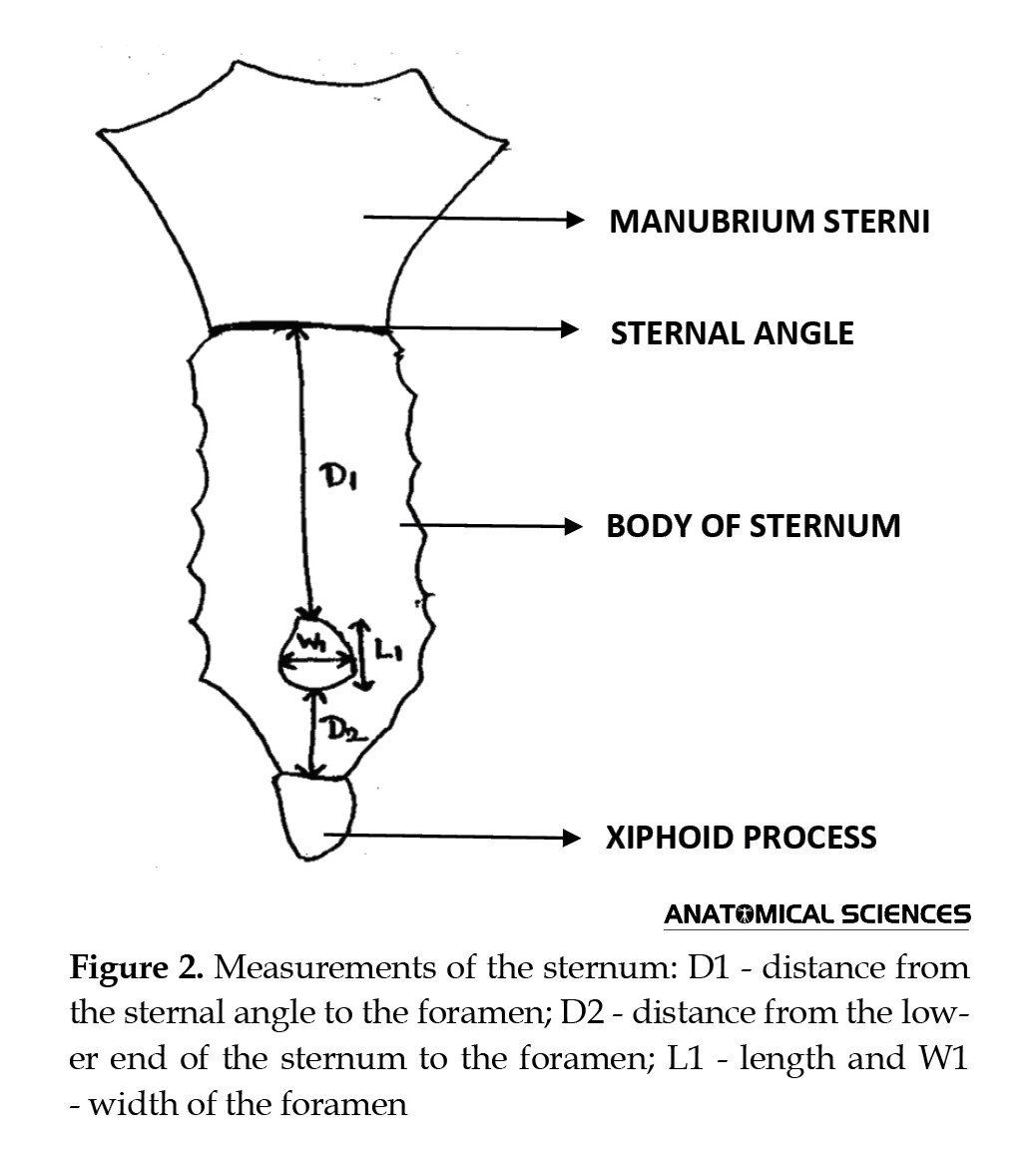
Measurements were recorded in three categories (Figure 2):
Length (L1) and width (W1) of the foramen; Distance from the sternal angle to the foramen (D1); Distance from the lower end of the sternum to the foramen (D2); All measurements were recorded in millimeters.
Results
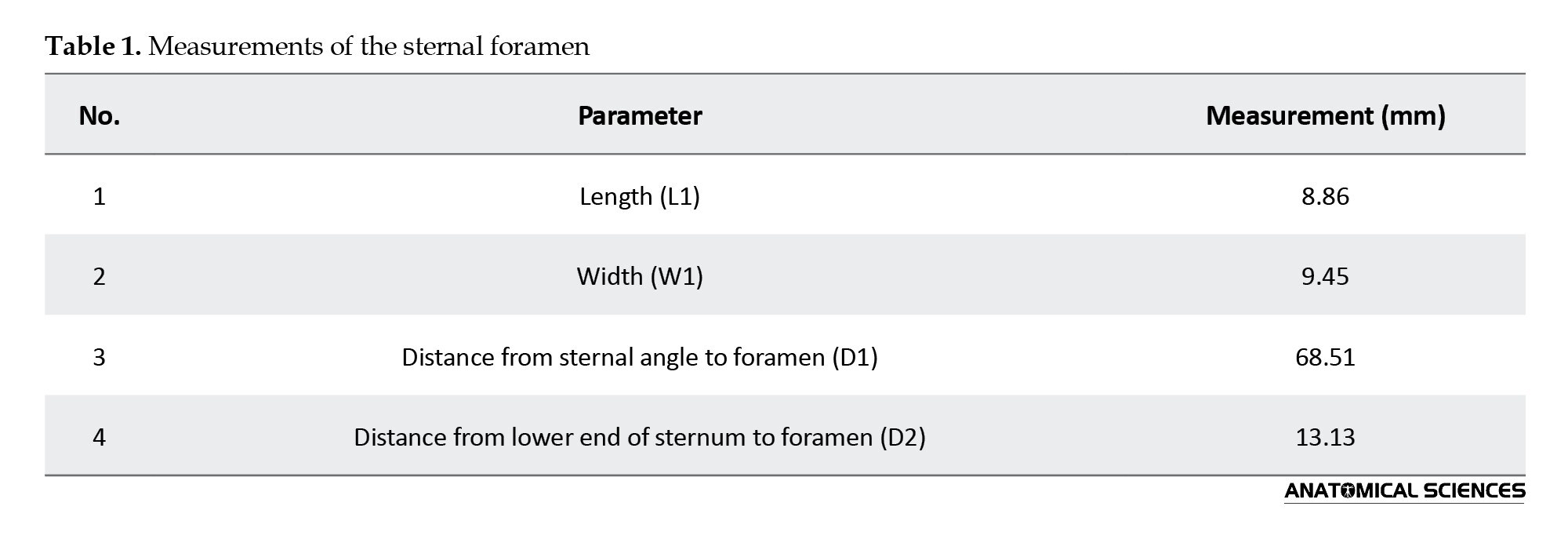
Among 100 sternums, 10% exhibited a sternal foramen. The foramen was oval, measuring 8.86 mm in length (L1) and 9.45 mm in width (W1). It was located in the lower third of the sternum, with a distance of 68.51 mm from the sternal angle (D1) and 13.13 mm from the lower end of the sternum (D2) (Table 1).
Discussion
The sternum is a flat, elongated bone forming the midline of the anterior thoracic wall. It consists of the manubrium, body, and xiphoid process. The manubrium sterni (prosternum) is quadrilateral and thick, positioned at the level of the T3 and T4 vertebrae. The body of the sternum (mesosternum) is longer, narrower, and thinner, formed by the fusion of four sternebrae. The xiphoid process (metasternum) is the smallest and terminates in a pointed caudal end. The sternal foramen results from incomplete ossification between the third and fourth sternebrae.
Previous studies have reported varying prevalence rates. Turkay et al. found sternal foramina in 5.2% of subjects using thoracic CT scans in 500 patients [5]. Paraskevas et al. reported a prevalence of 27.3% [6], while Boruah et al. found a prevalence of 11.6% in a study of 1,180 patients [7]. Kuzucuoglu and Albayrak analyzed 912 patients and reported an incidence of 8.44%, with 66.2% of foramina located in the sternal body [8]. These findings align with our study, where 10% of sternums exhibited a sternal foramen, located in the lower sternal body.
Tandon and Gara reported a sternal foramen measuring 8.75×7.35 mm, with distances of 68.06 mm from the sternal angle and 25.26 mm from the lower end of the sternum [9]. Suba and Reena reported larger measurements of 20.8×11.4 mm in the lower third of the sternum [10]. Our study found the sternal foramen to measure 8.86 mm in length and 9.45 mm in width, with distances of 68.51 mm from the sternal angle and 13.13 mm from the lower end of the sternum.
Conclusion
Although often asymptomatic, the sternal foramen poses a risk for complications during blind sternal procedures due to its proximity to vital thoracic structures. Additionally, it may lead to misinterpretation in radiological assessments. Awareness of this anatomical variation is crucial for healthcare providers to minimize potential complications.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Acknowledgments
The authors express gratitude to colleagues in the Department of Anatomy, Panimalar Medical College Hospital, and Research Institute, Chennai, India for their support and encouragement.
References
The sternal foramen results from incomplete fusion of the cartilaginous neonatal sternum and is typically found in the lower third of the sternal body. The average diameter of the foramen is 6.5 mm. This anatomical variation was first described by Eustachius in 1707 [1].
The sternum develops from the fusion of two cartilaginous plates along the mid-ventral line. It consists of three components: The manubrium, body, and xiphoid process. Ossification centers for the manubrium and first and second sternebrae appear in the 5th month of fetal life, while those for the third and fourth sternebrae typically appear in the fifth and sixth months, respectively. Fusion of the sternebrae begins at puberty and completes around the 25th year of life. A sternal foramen may occur between the third and fourth sternebrae due to ossification defects. Although often clinically insignificant, its presence must be considered during sternal interventions due to the underlying vital structures [2-4].
Patients with a sternal foramen are generally asymptomatic, often discovering the anomaly incidentally through radiological imaging or midline sternotomy. Awareness of the occurrence of sternal foramen is crucial for radiologists and surgeons. This study investigates the prevalence and anatomical characteristics of the sternal foramen.
Materials and Methods
A descriptive study was conducted on 100 adult sternums collected from the Department of Anatomy, Panimalar Medical College, Hospital, and Research Institute, Tamil Nadu, between April 2021 and April 2022. The presence of a fully formed sternal foramen was assessed visually by two independent investigators. Damaged or abnormally shaped sternums were excluded from the study.
The foramen was measured using a vernier caliper (Figure 1).
Measurements were recorded in three categories (Figure 2):
Length (L1) and width (W1) of the foramen; Distance from the sternal angle to the foramen (D1); Distance from the lower end of the sternum to the foramen (D2); All measurements were recorded in millimeters.
Results
Among 100 sternums, 10% exhibited a sternal foramen. The foramen was oval, measuring 8.86 mm in length (L1) and 9.45 mm in width (W1). It was located in the lower third of the sternum, with a distance of 68.51 mm from the sternal angle (D1) and 13.13 mm from the lower end of the sternum (D2) (Table 1).
Discussion
The sternum is a flat, elongated bone forming the midline of the anterior thoracic wall. It consists of the manubrium, body, and xiphoid process. The manubrium sterni (prosternum) is quadrilateral and thick, positioned at the level of the T3 and T4 vertebrae. The body of the sternum (mesosternum) is longer, narrower, and thinner, formed by the fusion of four sternebrae. The xiphoid process (metasternum) is the smallest and terminates in a pointed caudal end. The sternal foramen results from incomplete ossification between the third and fourth sternebrae.
Previous studies have reported varying prevalence rates. Turkay et al. found sternal foramina in 5.2% of subjects using thoracic CT scans in 500 patients [5]. Paraskevas et al. reported a prevalence of 27.3% [6], while Boruah et al. found a prevalence of 11.6% in a study of 1,180 patients [7]. Kuzucuoglu and Albayrak analyzed 912 patients and reported an incidence of 8.44%, with 66.2% of foramina located in the sternal body [8]. These findings align with our study, where 10% of sternums exhibited a sternal foramen, located in the lower sternal body.
Tandon and Gara reported a sternal foramen measuring 8.75×7.35 mm, with distances of 68.06 mm from the sternal angle and 25.26 mm from the lower end of the sternum [9]. Suba and Reena reported larger measurements of 20.8×11.4 mm in the lower third of the sternum [10]. Our study found the sternal foramen to measure 8.86 mm in length and 9.45 mm in width, with distances of 68.51 mm from the sternal angle and 13.13 mm from the lower end of the sternum.
Conclusion
Although often asymptomatic, the sternal foramen poses a risk for complications during blind sternal procedures due to its proximity to vital thoracic structures. Additionally, it may lead to misinterpretation in radiological assessments. Awareness of this anatomical variation is crucial for healthcare providers to minimize potential complications.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Acknowledgments
The authors express gratitude to colleagues in the Department of Anatomy, Panimalar Medical College Hospital, and Research Institute, Chennai, India for their support and encouragement.
References
- Choi PJ, Iwanaga J, Tubbis R. A comprehensive review of the sternal foramina and its clinical significance. Cureus. 2017; 9(12): e1929. [DOI:10.7759/cureus.1929]
- Datta AK. Essentials of human anatomy: Head & neck. Oakland: Current Books International; 2013. [Link]
- Vatzia K, Fanariotis M, Makridis KG, Vlychou M, Fezoulidis IV, Vassiou K. Frequency of sternal variations and anomalies in living individuals evaluated by MDCT. European Journal of Radiology. 2021; 142:109828. [DOI:10.1016/j.ejrad.2021.109828] [PMID]
- Babinski MA, De Lemos I, Babinski MS, Goncalues MV, De Paula RC, Fernandes RM. Frequency of sternal foramen evaluated by MDCT: A minor variation of great relevance. Surgical and Radiologic Anatomy. 2015; 37:287-91. [DOI:10.1007/s00276-014-1339-x] [PMID]
- Turkay R, Inci E, Ors S, Nalbant MO, Gurses IA. Frequency of sternal variations in living individuals. Surgical and Radiologic Anatomy. 2017; 39(11):1273-8. [DOI:10.1007/s00276-017-1854-7] [PMID]
- Paraskevas G, Tzika M, Anastasopoulos N, Kitsoulis P, Sofidis G, Natsis K. Sternal foramina: Incidence in Greek population, anatomy and clinical considerations. Surgical and Radiologic Anatomy. 2015; 37(7):845-51. [DOI:10.1007/s00276-014-1412-5] [PMID]
- Boruah DK, Prakash A, Yadav RR, Dhingani DD, Achar S, Augustine A, Mahanta K. The safe zone for blinded sternal interventions based on CT evaluation of midline congenital sternal foramina. Skeletal Radiology. 2016; 45(12):1619-28. [DOI:10.1007/s00256-016-2473-9] [PMID]
- Kuzucuoglu M, Albayrak I. Topographic evaluation of sternal foramen patients with thoracic computed tomography. Surgical and Radiologic Anatomy. 2020; 42(4):405-409. [DOI:10.1007/s00276-019-02416-3] [PMID]
- Tandon A, Gara RD. Sternal foramen. Medical Journal of DY Patil University. 2016; 9(1):127-8. [DOI:10.4103/0975-2870.167974]
- Kumarasamy SA, Agrawal R. A large sternal foramen. International Journal of Anatomical Variations. 2011; 4:195-6. [Link]
Type of Study: Original |
Subject:
Morphometry
Received: 2023/04/4 | Accepted: 2024/08/17 | Published: 2023/08/30
Received: 2023/04/4 | Accepted: 2024/08/17 | Published: 2023/08/30
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
