Sat, May 18, 2024
Volume 19, Issue 2 (Summer & Autumn 2022)
ASJ 2022, 19(2): 79-88 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Jahedi Zargar M, Heidari Keshel S, Kaviani S, Zahraei M, Izadyari Aghmiuni A, Savadkoohi A A, et al et al . Safety and efficacy of placental mesenchymal stem cell-derived extracellular vesicle in severe COVID-19 patients: Phase I & II Clinical Trials. ASJ 2022; 19 (2) :79-88
URL: http://anatomyjournal.ir/article-1-585-en.html
URL: http://anatomyjournal.ir/article-1-585-en.html
Mehdi Jahedi Zargar1 
 , Saeed Heidari Keshel2
, Saeed Heidari Keshel2  , Saeid Kaviani1 , Mohammad Zahraei3 , Azadeh Izadyari Aghmiuni4 , Ali Amir Savadkoohi5 , Hamidreza Jamaati6 , Mohammad Samet7 , Mahsa Soufizomorrod8 , Mina Soufi Zomorrod9 , Faeze Sadat Heidari10 , Mohamad Reza Mirjalili11 , Payam Tabarsi12 , Mohammadreza Soroush3 , Rasoul Aliannejad13 , Mojtaba Javani14 , Hosein Shafiii14 , Mohammad Vasei15 , Masoud Soleimani 2
, Saeid Kaviani1 , Mohammad Zahraei3 , Azadeh Izadyari Aghmiuni4 , Ali Amir Savadkoohi5 , Hamidreza Jamaati6 , Mohammad Samet7 , Mahsa Soufizomorrod8 , Mina Soufi Zomorrod9 , Faeze Sadat Heidari10 , Mohamad Reza Mirjalili11 , Payam Tabarsi12 , Mohammadreza Soroush3 , Rasoul Aliannejad13 , Mojtaba Javani14 , Hosein Shafiii14 , Mohammad Vasei15 , Masoud Soleimani 2
, Saeed Heidari Keshel2 , Saeid Kaviani1 , Mohammad Zahraei3 , Azadeh Izadyari Aghmiuni4 , Ali Amir Savadkoohi5 , Hamidreza Jamaati6 , Mohammad Samet7 , Mahsa Soufizomorrod8 , Mina Soufi Zomorrod9 , Faeze Sadat Heidari10 , Mohamad Reza Mirjalili11 , Payam Tabarsi12 , Mohammadreza Soroush3 , Rasoul Aliannejad13 , Mojtaba Javani14 , Hosein Shafiii14 , Mohammad Vasei15 , Masoud Soleimani 2
1- Department of Hematology, Faculty of Medical Science, Tarbiat Modares University, Tehran, Iran.
2- Department of Tissue Engineering and Applied Cell Science, School of Advanced Technologies in Medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
3- Nikan Education & Research center (NERC), West Nikan Hospital, Tehran, Iran.
4- Department of Nanobiotechnology, Pasteur Institute of Iran, Tehran, Iran.
5- Department of Anesthesia and Critical Care, Mehrad Hospital, Tehran, Iran.
6- Chronic Respiratory Diseases Research Center (CRDRC), National Research Institute of Tuberculosis and Lung Diseases (NRITLD), Shahid Beheshti University of Medical Sciences, Tehran, Iran.
7- Department of Internal Medicine, Shahid Sadoughi Hospital, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
8- National Institute of Genetic Engineering and Biotechnology (NIGEB), Tehran, Iran.
9- Department of Applied Cell Science and Hematology, Faculty of Medical Science, Tarbiat Modares University, Tehran, Iran.
10- Department of Infectious Diseases, Infectious Diseases Research Center, School of Medicine, Shahid Sadoughi General Hospital, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
11- Department of Anesthesia and Intensive Care Medicine, Faculty of Medicine, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
12- Clinical Tuberculosis and Epidemiology Research Center, National Research Institute of Tuberculosis and Lung Diseases (NRITLD), Shahid Beheshti University of Medical Sciences, Tehran, Iran.
13- Department of Pulmonary, Shariati Hospital, Tehran University of Medical Sciences, Tehran, Iran.
14- Shahid Sadughi Hospital, Isfahan, Iran.
15- Cell Therapy Based Research Center, Digestive Disease Research Institute, Shariati Hospital, Tehran University of Medical Science, Tehran, Iran.
2- Department of Tissue Engineering and Applied Cell Science, School of Advanced Technologies in Medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
3- Nikan Education & Research center (NERC), West Nikan Hospital, Tehran, Iran.
4- Department of Nanobiotechnology, Pasteur Institute of Iran, Tehran, Iran.
5- Department of Anesthesia and Critical Care, Mehrad Hospital, Tehran, Iran.
6- Chronic Respiratory Diseases Research Center (CRDRC), National Research Institute of Tuberculosis and Lung Diseases (NRITLD), Shahid Beheshti University of Medical Sciences, Tehran, Iran.
7- Department of Internal Medicine, Shahid Sadoughi Hospital, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
8- National Institute of Genetic Engineering and Biotechnology (NIGEB), Tehran, Iran.
9- Department of Applied Cell Science and Hematology, Faculty of Medical Science, Tarbiat Modares University, Tehran, Iran.
10- Department of Infectious Diseases, Infectious Diseases Research Center, School of Medicine, Shahid Sadoughi General Hospital, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
11- Department of Anesthesia and Intensive Care Medicine, Faculty of Medicine, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
12- Clinical Tuberculosis and Epidemiology Research Center, National Research Institute of Tuberculosis and Lung Diseases (NRITLD), Shahid Beheshti University of Medical Sciences, Tehran, Iran.
13- Department of Pulmonary, Shariati Hospital, Tehran University of Medical Sciences, Tehran, Iran.
14- Shahid Sadughi Hospital, Isfahan, Iran.
15- Cell Therapy Based Research Center, Digestive Disease Research Institute, Shariati Hospital, Tehran University of Medical Science, Tehran, Iran.
Keywords: COVID‐19, Extracellular vesicles, Mesenchymal stromal cell, Placenta-derived mesenchymal stem cell, Acute respiratory distress syndrome
Full-Text [PDF 2257 kb]
(117 Downloads)
| Abstract (HTML) (471 Views)

Full-Text: (133 Views)
1. Introduction
Since December 2019, coronavirus disease-2019 (COVID-19) caused by SARS coronavirus 2 (SARS-CoV-2) infections have spread rapidly across the globe and declared a global pandemic by the World Health Organization (WHO). While most patients experience mild symptoms like fever and dry cough [1], others go through more severe complications like acute respiratory distress syndrome, which may lead to intubation and death [2].
The reports indicate that chronic inflammation caused by COVID-19 is related to increased pro-inflammatory cytokines, acute-phase proteins, viral invasion of lymphocytes, activation of macrophages, and oxidative stress. Moreover, it can exacerbate and dysregulate immune responses. Hence, uncontrolled inflammation can lead to severe/irreversible damage to the respiratory tract, kidneys, liver, and heart [3].
Mesenchymal stem cells (MSCs) are multipotent progenitors capable of differentiating into various cell types [4]. Based on the studies, using MSCs is beneficial in decreasing inflammation due to their immunomodulatory characteristics [5]. The anti-inflammatory property of these cells is performed via stimulating the toll-like receptors by viral RNAs, leading to an inhibitory effect on the dendritic cells, lymphocytes, neutrophils, and monocytes [6]. Moreover, it can be isolated from various tissues and retain damaged tissue regeneration by migrating to the site of injury and differentiation [7]. Studies demonstrate that using MSCs for deregulated immune responses, cytokine storms, and lung injuries caused by COVID-19 can be a promising strategy [8, 9, 10, 11]. The challenges of stem cell therapy, such as cellular survivability and scalability, limit the extensive use of MSCs, leading researchers to introduce an alternative for benefiting their properties without using the cellular compartment [12, 13].
MSCs-derived extracellular vesicles (EVs) are novel biological agents that can significantly reduce inflammation and cytokine storm caused by COVID-19. Indeed, extracellular vesicles possess immunomodulatory and anti-inflammatory functions due to their cargo of growth factors, micro-RNAs, mRNA, and chemokines [14]. Moreover, their scalability, stability, and safety have made these vesicles practical therapeutic options for COVID-19 disease [15]. Many studies on animal models in this field indicate that MSCs-derived vesicles are essential in decreasing acute lung injuries and inflammatory diseases [16].
The present study focused on the therapeutic effects of placental mesenchymal stem cell (PMSC)-derived vesicles on the inflammation and pulmonary injury caused by COVID-19 disease.
2. Materials and Methods
Placental mesenchymal stem cells-derived vesicle preparation
Passage-3 of placenta-derived mesenchymal stem cells was obtained from our previous study [17]. After cell culture in serum-free DMEM containing GlutamaX, NEAA, and penicillin/
Streptomycin medium and incubated in 5% CO2 at 370C for 72 hours. The conditioned culture media was collected and centrifuged at 300 for 10 minutes. The obtained cell suspension was re-centrifuged at 20000 g for 10 minutes and then 10000 g for 30 minutes to remove dead cells, cell debris, and large particles. The supernatant was ultra-centrifuged using a W32Ti rotor (L-80XP; Beckman Coulter, USA) at 110000 g for 70 minutes to pellet the vesicles. The pellet was washed in phosphate-buffered saline (PBS) (Sigma-Aldrich, USA) and centrifuged again at 110000 g for 70 minutes to eliminate contaminating proteins. Finally, the vesicles were re-suspended in 100 µL sodium chloride 0.9% (Sigma-Aldrich, USA) for intravenous infusion.
Vesicle characteristics
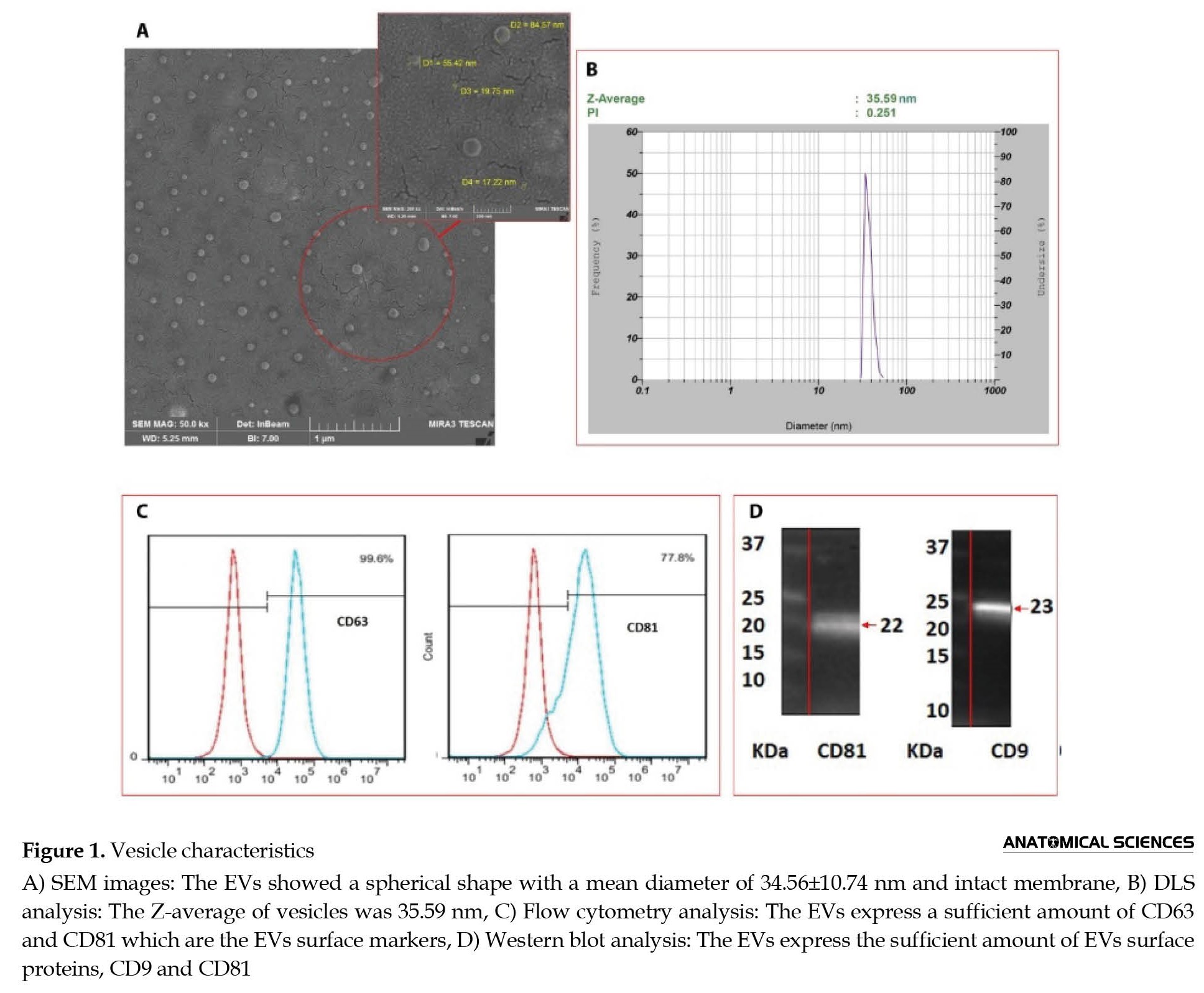
The morphology assessment of the vesicles was performed by a scanning electron microscope using Philips XL30 SEM) (Germany). The vesicles were imaged at an accelerating voltage of 20.0 kV, and the mean diameter was measured by Clemex Vision software with at least 100 vesicles. Dynamic light scattering (DLS) measurement was carried out to study the size distribution of vesicles using an SZ-100 Nanopartica Series Instrument (Horiba, Japan), with a dynamic range of 0.3 nm–8 µm and scattering angle of 90°.
The flow cytometric test was performed using anti-CD81and anti-CD63 monoclonal antibodies (Abcam Co, UK) and FACScan Becton Dickinson device (BD Biosciences, USA) and analyzed using flowing software-2.5.1 (BD Company, USA). The western blot assay was performed using anti-CD9 and anti-CD81 (Abcam, UK) and observed using an increased chemiluminescence kit (Bio-Rad, USA) using Chemidoc Touch (Bio-Rad, USA). CD9 and CD81 are the surface proteins expressed on the outer membrane of the EVs [18].
Clinical trial
From April 2021 to August 2021, the study was carried out in phases I and II to evaluate the safety and efficiency of PMSC-derived EVs. COVID-19 patients admitted to four hospital centers (Shahid Sadoughi University of Medical Sciences and Health Services, Yazd, Iran; Shariati Hospital, Tehran, Iran; Noor Afshar Hospital, Tehran, Iran; and West Nikan Hospital, Tehran, Iran) were enrolled in a blinded randomized, double-blind study. Inclusion criteria included age 20–75 years, positive SARS-CoV-2 polymerase chain reaction results, patient clinical deterioration, and down-trending in peripheral blood oxygen saturation (SpO2). Exclusion criteria involved pregnancy, body weight index higher than 35, chronic heart failure, and severe pre-existing pulmonary, hepatic, or renal disease. Written informed consent was obtained from patients or their families. Initial screening involved reviewing medical histories, physical examinations and monitoring vital signs during hospitalization. The treatment was applied to patients with severe COVID-19 hospitalized in the intensive care unit; among them, 15 cases were intubated, 15 were on non-invasive ventilation (NIV) and 2 received oxygen with a reserve bag. The intervention was not initiated until the patient reached a stable condition.
Administration dose and route
As Hashemian et al. [17] confirmed that multiple infusions of high-dose allogeneic prenatal MSCs are safe and can rapidly improve respiratory distress and reduce inflammatory biomarkers in some severe COVID-19-induced ARDS cases, we determined the optimum dose based on that study, in which patient received intravenous infusions of a total dose of 600×106 allogeneic human MSCs in three doses every other day. In the present study, 1800×106 MSCs were cultured, and the released EVs were isolated. A total number of 1×1011±10% vesicles were obtained, dissolved in 100 mL of sterile sodium chloride 0.9% (normal saline) solution. For five consecutive days, in addition to standard treatments, 15 mL (1×109 vesicles/1 mL) of the solution, which contained a total of 15×109 vesicles, was injected intravenously with an injection rate of 4-5 mL/minute.
Vital signs assessments and baseline tests
In phase I, the respiratory, hepatic, and cardiac system function, consciousness level, hemoglobin level, white blood cell count, pulse rate, respiratory rate, ferritin, creatinine, blood urea nitrogen (BUN), C-reactive protein (CRP) levels, partial Thromboplastin time, platelet-lymphocyte ratio, and neutrophil-lymphocyte ratio (NLR), were performed before infusion and also on minutes 10, 30, 60, on the hour 12 h, and on days 6, 7, 14, and 28 after the first infusion. Chest x-rays were performed on day zero (before intervention) and on days 1-5 (from the first day after the intervention to the fifth day of it).
In phase II (efficacy assessment), all the mentioned tests were performed on the days of treatment. The axial chest CT scan was scored following the involvement percentage of lung lobes (A<5%, B: 5–30%, C: 31–50%, D: 51–80%, and E>80%).
Statistical analysis
Statistical analysis was performed using the t-test and one-way analysis of variance (one-way ANOVA, Tukey-test) and two-way ANOVA by GraphPad Prism software, version 6. Data were calculated using three measurements and were expressed as Mean±SD.
3. Results
Vesicle characteristics
The vesicles’ morphology, diameter, and size distribution were evaluated using SEM images and the DLS method. As shown in Figure 1A, the vesicles showed a spherical shape with a mean diameter of 34.56±10.74 nm (min: 13.79 nm, max: 84.57 nm), confirming the structure of extracellular vesicles.
Since December 2019, coronavirus disease-2019 (COVID-19) caused by SARS coronavirus 2 (SARS-CoV-2) infections have spread rapidly across the globe and declared a global pandemic by the World Health Organization (WHO). While most patients experience mild symptoms like fever and dry cough [1], others go through more severe complications like acute respiratory distress syndrome, which may lead to intubation and death [2].
The reports indicate that chronic inflammation caused by COVID-19 is related to increased pro-inflammatory cytokines, acute-phase proteins, viral invasion of lymphocytes, activation of macrophages, and oxidative stress. Moreover, it can exacerbate and dysregulate immune responses. Hence, uncontrolled inflammation can lead to severe/irreversible damage to the respiratory tract, kidneys, liver, and heart [3].
Mesenchymal stem cells (MSCs) are multipotent progenitors capable of differentiating into various cell types [4]. Based on the studies, using MSCs is beneficial in decreasing inflammation due to their immunomodulatory characteristics [5]. The anti-inflammatory property of these cells is performed via stimulating the toll-like receptors by viral RNAs, leading to an inhibitory effect on the dendritic cells, lymphocytes, neutrophils, and monocytes [6]. Moreover, it can be isolated from various tissues and retain damaged tissue regeneration by migrating to the site of injury and differentiation [7]. Studies demonstrate that using MSCs for deregulated immune responses, cytokine storms, and lung injuries caused by COVID-19 can be a promising strategy [8, 9, 10, 11]. The challenges of stem cell therapy, such as cellular survivability and scalability, limit the extensive use of MSCs, leading researchers to introduce an alternative for benefiting their properties without using the cellular compartment [12, 13].
MSCs-derived extracellular vesicles (EVs) are novel biological agents that can significantly reduce inflammation and cytokine storm caused by COVID-19. Indeed, extracellular vesicles possess immunomodulatory and anti-inflammatory functions due to their cargo of growth factors, micro-RNAs, mRNA, and chemokines [14]. Moreover, their scalability, stability, and safety have made these vesicles practical therapeutic options for COVID-19 disease [15]. Many studies on animal models in this field indicate that MSCs-derived vesicles are essential in decreasing acute lung injuries and inflammatory diseases [16].
The present study focused on the therapeutic effects of placental mesenchymal stem cell (PMSC)-derived vesicles on the inflammation and pulmonary injury caused by COVID-19 disease.
2. Materials and Methods
Placental mesenchymal stem cells-derived vesicle preparation
Passage-3 of placenta-derived mesenchymal stem cells was obtained from our previous study [17]. After cell culture in serum-free DMEM containing GlutamaX, NEAA, and penicillin/
Streptomycin medium and incubated in 5% CO2 at 370C for 72 hours. The conditioned culture media was collected and centrifuged at 300 for 10 minutes. The obtained cell suspension was re-centrifuged at 20000 g for 10 minutes and then 10000 g for 30 minutes to remove dead cells, cell debris, and large particles. The supernatant was ultra-centrifuged using a W32Ti rotor (L-80XP; Beckman Coulter, USA) at 110000 g for 70 minutes to pellet the vesicles. The pellet was washed in phosphate-buffered saline (PBS) (Sigma-Aldrich, USA) and centrifuged again at 110000 g for 70 minutes to eliminate contaminating proteins. Finally, the vesicles were re-suspended in 100 µL sodium chloride 0.9% (Sigma-Aldrich, USA) for intravenous infusion.
Vesicle characteristics
The morphology assessment of the vesicles was performed by a scanning electron microscope using Philips XL30 SEM) (Germany). The vesicles were imaged at an accelerating voltage of 20.0 kV, and the mean diameter was measured by Clemex Vision software with at least 100 vesicles. Dynamic light scattering (DLS) measurement was carried out to study the size distribution of vesicles using an SZ-100 Nanopartica Series Instrument (Horiba, Japan), with a dynamic range of 0.3 nm–8 µm and scattering angle of 90°.
The flow cytometric test was performed using anti-CD81and anti-CD63 monoclonal antibodies (Abcam Co, UK) and FACScan Becton Dickinson device (BD Biosciences, USA) and analyzed using flowing software-2.5.1 (BD Company, USA). The western blot assay was performed using anti-CD9 and anti-CD81 (Abcam, UK) and observed using an increased chemiluminescence kit (Bio-Rad, USA) using Chemidoc Touch (Bio-Rad, USA). CD9 and CD81 are the surface proteins expressed on the outer membrane of the EVs [18].
Clinical trial
From April 2021 to August 2021, the study was carried out in phases I and II to evaluate the safety and efficiency of PMSC-derived EVs. COVID-19 patients admitted to four hospital centers (Shahid Sadoughi University of Medical Sciences and Health Services, Yazd, Iran; Shariati Hospital, Tehran, Iran; Noor Afshar Hospital, Tehran, Iran; and West Nikan Hospital, Tehran, Iran) were enrolled in a blinded randomized, double-blind study. Inclusion criteria included age 20–75 years, positive SARS-CoV-2 polymerase chain reaction results, patient clinical deterioration, and down-trending in peripheral blood oxygen saturation (SpO2). Exclusion criteria involved pregnancy, body weight index higher than 35, chronic heart failure, and severe pre-existing pulmonary, hepatic, or renal disease. Written informed consent was obtained from patients or their families. Initial screening involved reviewing medical histories, physical examinations and monitoring vital signs during hospitalization. The treatment was applied to patients with severe COVID-19 hospitalized in the intensive care unit; among them, 15 cases were intubated, 15 were on non-invasive ventilation (NIV) and 2 received oxygen with a reserve bag. The intervention was not initiated until the patient reached a stable condition.
Administration dose and route
As Hashemian et al. [17] confirmed that multiple infusions of high-dose allogeneic prenatal MSCs are safe and can rapidly improve respiratory distress and reduce inflammatory biomarkers in some severe COVID-19-induced ARDS cases, we determined the optimum dose based on that study, in which patient received intravenous infusions of a total dose of 600×106 allogeneic human MSCs in three doses every other day. In the present study, 1800×106 MSCs were cultured, and the released EVs were isolated. A total number of 1×1011±10% vesicles were obtained, dissolved in 100 mL of sterile sodium chloride 0.9% (normal saline) solution. For five consecutive days, in addition to standard treatments, 15 mL (1×109 vesicles/1 mL) of the solution, which contained a total of 15×109 vesicles, was injected intravenously with an injection rate of 4-5 mL/minute.
Vital signs assessments and baseline tests
In phase I, the respiratory, hepatic, and cardiac system function, consciousness level, hemoglobin level, white blood cell count, pulse rate, respiratory rate, ferritin, creatinine, blood urea nitrogen (BUN), C-reactive protein (CRP) levels, partial Thromboplastin time, platelet-lymphocyte ratio, and neutrophil-lymphocyte ratio (NLR), were performed before infusion and also on minutes 10, 30, 60, on the hour 12 h, and on days 6, 7, 14, and 28 after the first infusion. Chest x-rays were performed on day zero (before intervention) and on days 1-5 (from the first day after the intervention to the fifth day of it).
In phase II (efficacy assessment), all the mentioned tests were performed on the days of treatment. The axial chest CT scan was scored following the involvement percentage of lung lobes (A<5%, B: 5–30%, C: 31–50%, D: 51–80%, and E>80%).
Statistical analysis
Statistical analysis was performed using the t-test and one-way analysis of variance (one-way ANOVA, Tukey-test) and two-way ANOVA by GraphPad Prism software, version 6. Data were calculated using three measurements and were expressed as Mean±SD.
3. Results
Vesicle characteristics
The vesicles’ morphology, diameter, and size distribution were evaluated using SEM images and the DLS method. As shown in Figure 1A, the vesicles showed a spherical shape with a mean diameter of 34.56±10.74 nm (min: 13.79 nm, max: 84.57 nm), confirming the structure of extracellular vesicles.
The DLS results also demonstrated that the Z-average of vesicles was 35.59 nm with a PDI (polydispersity index) of 0.251 (Figure 1B). Flow cytometric analysis indicated sufficient CD63 and CD81 signals (Figure 1C). CD63 and CD81 were expressed at higher levels than 98% and 75%, respectively. The Western blot results also confirmed the presence of extracellular vesicles (CD9 and CD81) (Figure 1D).
Clinical characteristics of patients
Among 101 patients enrolled in phase I of the study, 63% and 37% were male and female, respectively. The age range was 36–75 years, averaging 54. The mortality rate and hospitalization period were 23% and 11 days, respectively. A total number of 80 cases were enrolled in phase II, divided into intervention and control groups (40 in each group). Besides, among 40 patients enrolled in the intervention group of phase II, 60% and 40% were female, with an age range of 38–75 years (average age: 54). In this group, the mortality rate and hospitalization period were 25% (8 subjects) and 14 days, respectively. The control group of phase II included 40 cases, 61% male and 39% female, with an age range of 36–72 years (with an average of 52 years). The mortality rate and hospitalization period were 33% (4 subjects) and 12 days, respectively.
Safety assessment
No intervention-related reaction or adverse events were observed in any patient (n=101) during the infusions. The improvement in respiratory rate was observed in two subjects. The paraclinical assessments (hemoglobin, coagulation factors, inflammatory parameters, renal, respiratory, and cardiovascular functions based on pulse rate, SpO2, and chest x-ray) showed no side effects, except for three patients who showed a significant rise in creatinine levels, although two of them showed increased creatinine levels even before injection. No drug-drug interaction or reduced drug effect was observed.
Efficacy study
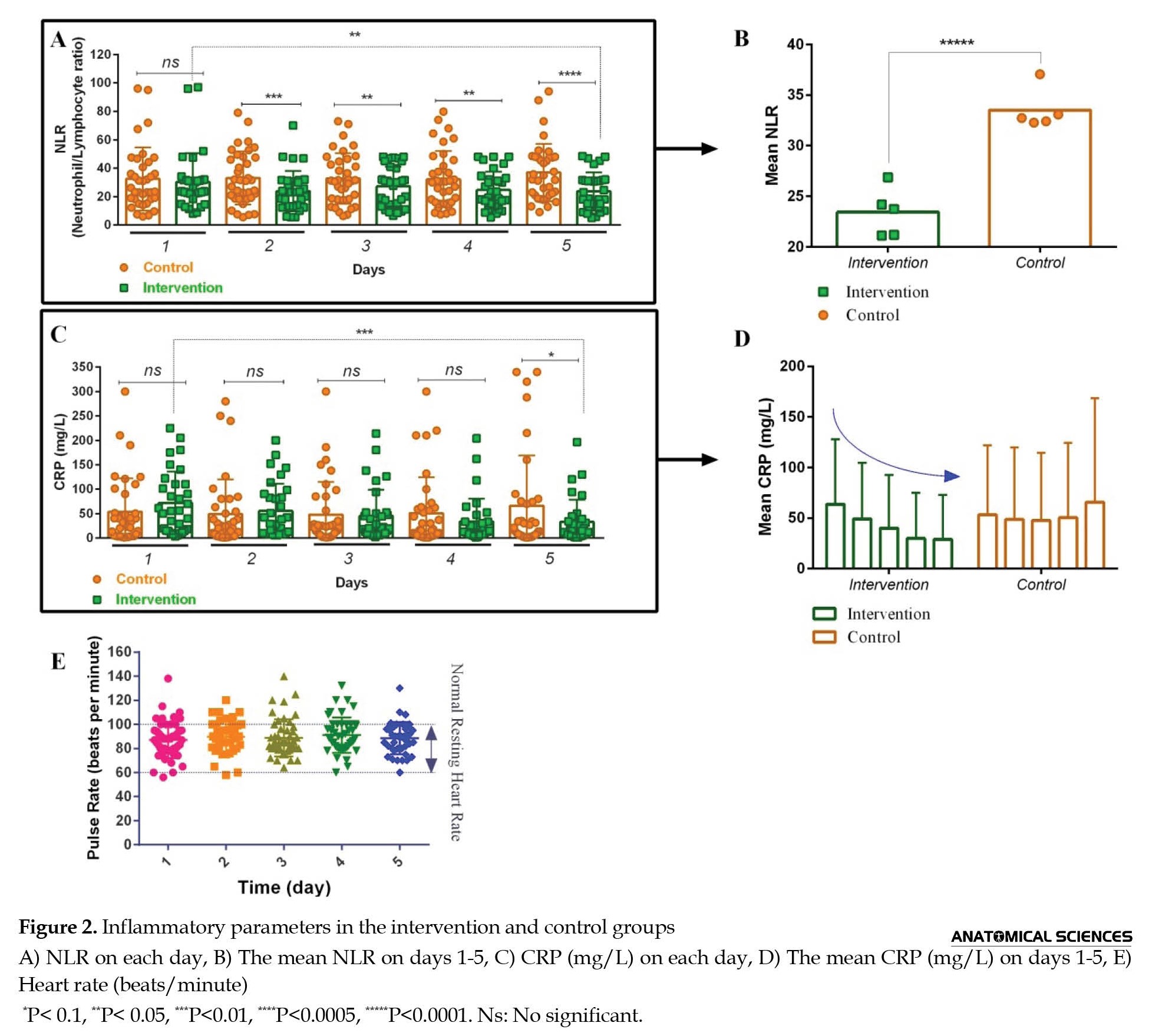
Inflammatory factors: Results indicated a significant difference in NLR between the control and intervention groups on each day (Figure 2A).
Clinical characteristics of patients
Among 101 patients enrolled in phase I of the study, 63% and 37% were male and female, respectively. The age range was 36–75 years, averaging 54. The mortality rate and hospitalization period were 23% and 11 days, respectively. A total number of 80 cases were enrolled in phase II, divided into intervention and control groups (40 in each group). Besides, among 40 patients enrolled in the intervention group of phase II, 60% and 40% were female, with an age range of 38–75 years (average age: 54). In this group, the mortality rate and hospitalization period were 25% (8 subjects) and 14 days, respectively. The control group of phase II included 40 cases, 61% male and 39% female, with an age range of 36–72 years (with an average of 52 years). The mortality rate and hospitalization period were 33% (4 subjects) and 12 days, respectively.
Safety assessment
No intervention-related reaction or adverse events were observed in any patient (n=101) during the infusions. The improvement in respiratory rate was observed in two subjects. The paraclinical assessments (hemoglobin, coagulation factors, inflammatory parameters, renal, respiratory, and cardiovascular functions based on pulse rate, SpO2, and chest x-ray) showed no side effects, except for three patients who showed a significant rise in creatinine levels, although two of them showed increased creatinine levels even before injection. No drug-drug interaction or reduced drug effect was observed.
Efficacy study
Inflammatory factors: Results indicated a significant difference in NLR between the control and intervention groups on each day (Figure 2A).
While the intervention led to a 21% decrease in NLR on day five compared to day one, it increased by 14% in the control group. The comparison of the mean NLR of both groups during five days demonstrated a 21.36% decrease in the intervention group compared to the control group (Figure 2B).
CRP results illustrated no significant difference between the control and intervention groups on days 1-4 (Figure 2C). In contrast, after day five, CRP decreased by 54.23 % in the intervention group and increased by 23% in the control group (Figure 2D).
Cardiovascular function: Pulse rate results showed a normal resting heart rate (60-100 beats/minute) after five days in 87.5% of patients (Figure 2E).
Kidney and liver function: Creatinine and BUN results, showing a 1% reduction in the intervention group, indicated that the intervention had no side effects on the kidney. In contrast, in the control group, after five days, an increase of ~27.5% and ~43% was observed in creatinine and BUN values, respectively (Figure 3A-D).
CRP results illustrated no significant difference between the control and intervention groups on days 1-4 (Figure 2C). In contrast, after day five, CRP decreased by 54.23 % in the intervention group and increased by 23% in the control group (Figure 2D).
Cardiovascular function: Pulse rate results showed a normal resting heart rate (60-100 beats/minute) after five days in 87.5% of patients (Figure 2E).
Kidney and liver function: Creatinine and BUN results, showing a 1% reduction in the intervention group, indicated that the intervention had no side effects on the kidney. In contrast, in the control group, after five days, an increase of ~27.5% and ~43% was observed in creatinine and BUN values, respectively (Figure 3A-D).
Albumin results illustrated that its level was in the range of 3.3-5 g/dl in all patients before and after five days (Figure 3F), indicating that the intervention did not deteriorate kidney and liver function.
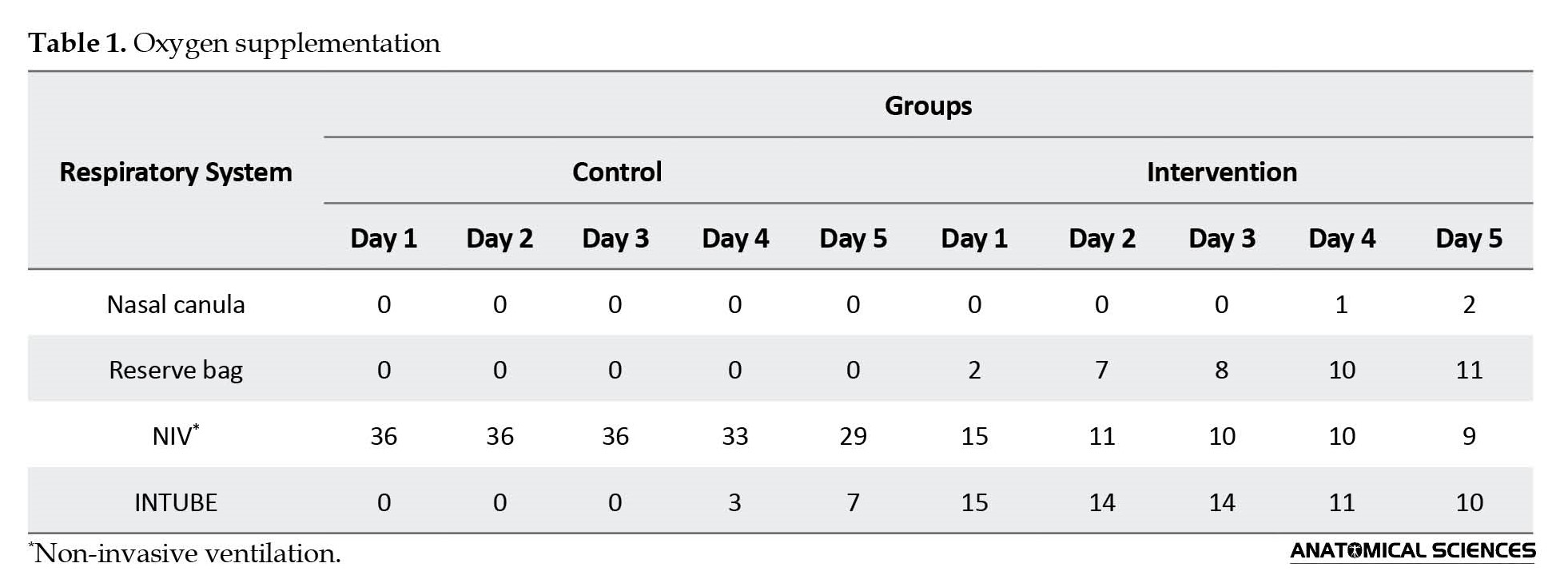
Oxygen supplementation: The SpO2 results demonstrated that after 5 days, from 32 patients in the intervention group, the SpO2 level of 24 patients (75%) increased compared to day one (Figure 3E). Moreover, the number of intubated patients decreased from 15 to 10 subjects (Table 1).
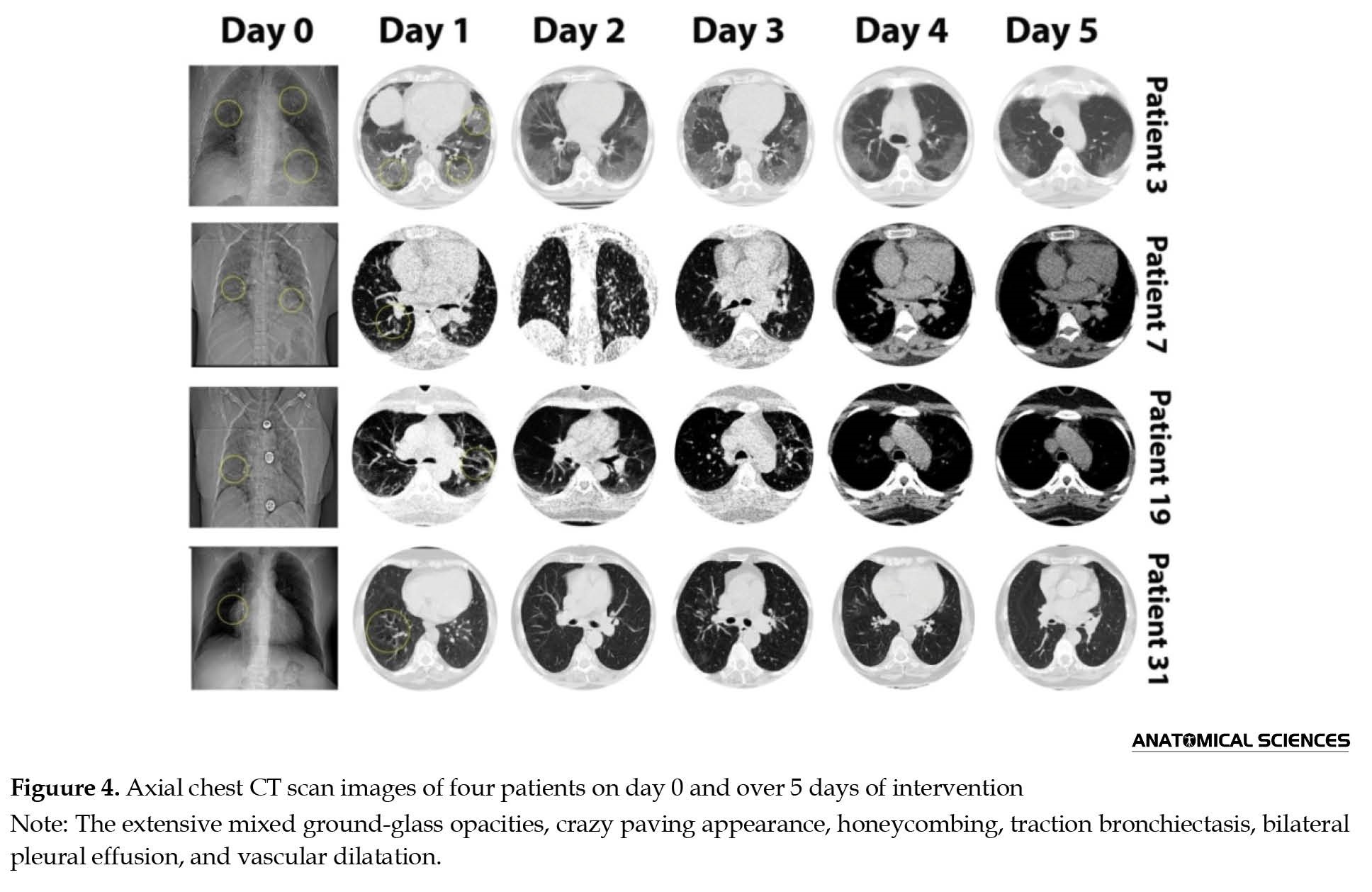
Lung function: Day zero chest x-ray demonstrated a significant lung involvement in all patients, varied from mixed ground-glass opacity, crazy paving patterns, vascular dilation, pleural effusion, honeycombing, and traction bronchiectasis. After five days of intervention, a significant improvement was observed in the chest x-ray images (Figure 4).
Oxygen supplementation: The SpO2 results demonstrated that after 5 days, from 32 patients in the intervention group, the SpO2 level of 24 patients (75%) increased compared to day one (Figure 3E). Moreover, the number of intubated patients decreased from 15 to 10 subjects (Table 1).
Lung function: Day zero chest x-ray demonstrated a significant lung involvement in all patients, varied from mixed ground-glass opacity, crazy paving patterns, vascular dilation, pleural effusion, honeycombing, and traction bronchiectasis. After five days of intervention, a significant improvement was observed in the chest x-ray images (Figure 4).
Five out of 15 (~34%) intubated patients and six of 14(40%) non-invasive ventilation-supported patients recovered. A 4.5-fold increase was observed in the number of patients supported by reserve bags.
4. Discussion
Cytokine storm is a lethal systemic inflammatory syndrome defined by hyperactivated immune cells and increased circulating inflammatory cytokines and chemical mediators [19]. It is responsible for the disease severity and mortality in COVID-19 patients [20]. Various studies revealed that severe COVID-19 patients showed higher levels of pro-inflammatory and inflammatory cytokines compared to patients with mild and moderate infections. Hence, early control of the cytokine storm is critical in improving their survival rate [21]. Among the cytokine storm-attenuating therapies, MSC therapy exhibited a promising potential for rapid and significant improvement in clinical symptoms [22].
Due to the immunomodulatory properties of MSCs [23], they attract lots of attention during the pandemic [24-26]. Various studies have evaluated the safety and efficacy of MSCs in severe COVID-19 management (111 clinical trials until October 2022). Also, there are some clinical trials registered on ClinicalTrials data base, applying MSC-derived EVs (NCT05216562, NCT05191381, NCT04798716, NCT04602442, NCT04491240, NCT04493242) or placenta-derived MSCs (NCT04461925, NCT04614025, NCT04389450) in COVID-19. There is just one study (NCT05387278) that evaluated the PMSC-derived EVs in severe COVID-19 conditions, and no data published yet. In agreement with the mentioned clinical trials utilizing MSCs or MSC-derived EVs [27], we detected no intervention-related adverse effects during or after the infusions.
Liu et al. compared severe COVID-19 patients with mild patients and reported a significant and persistent decline in T helper and T cytotoxic lymphocyte counts, contrary to the increase in neutrophils. Therefore, the NLR is a predictive biomarker for COVID-19 outcomes [28]. In agreement with previous studies, NLR results demonstrated a decrease in the intervention group and an increase in the control group. The NLR downtrend through the intervention indicates the treatment’s effectiveness.
CRP is an acute-phase protein that increases in infection or inflammation conditions and serves as a predictive biomarker in COVID-19 patients [29]. Ahnach et al. claimed that CRP level was significantly related to COVID-19 severity [29]. Besides, as CRP indicated the presence of systemic inflammation, Smilowitz et al. suggested that a high level of serum CRP is intensely related to morbidity and mortality in COVID-19 patients [30]. In the present study, CRP decreased in the intervention group and increased in the control group. Hence, the intervention is supposed to be effective in severe COVID-19 patients.
Increased serum creatinine and BUN are independent predictors of severe COVID-19 [31]. Although the increased creatinine level even before the intervention suggested that it was probably due to the COVID-19 infection, the decreased glomerular filtration of EVs and their possible aggregation can also lead to closure and increased creatinine levels.
Fathi-Kazerooni et al. applied MSC-derived Evs from allogeneic menstrual blood in severe COVID-19. Similar to our study, they detected no adverse events following three days of intervention. Also, they reported a significant decrease in CRP after the intervention. Also, consistent with our study, they reported a significant improvement in lymphopenia. Consistently with our findings, they demonstrated that five consecutive doses of MSC-derived secretome improved hypoxia, lessened pulmonary lesions, restored the immune system function, and eased the cytokine storm in severe COVID-19 [32].
Sengupta et al. conducted a cohort study that assessed the safety and efficacy of a single dose of intravenous EVs derived from allogeneic bone marrow MSCs in severe COVID-19. They concluded that EVs from bone marrow MSCs could restore oxygenation, down-regulating cytokine storm, and re-constituting immunity. In accordance with this cohort study, our findings illustrated that applying the MSC-derived EVs can increase SpO2, improve lung injuries, and alleviate cytokine storms [33].
5. Conclusions
Generally, this study demonstrated that intravenous infusion of PMSC-derived EVs decreased cytokine storms, improved pulmonary function, and decreased invasive oxygen/mechanical ventilation support in hospitalized patients with severe COVID-19, with no associated side effects.
Ethical Considerations
Compliance with ethical guidelines
The clinical trial was approved by the Ethics Committee of the Tehran University of Medical Sciences (Code: IR.TUMS.MEDICINE.REC.1399.454).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors would like to thank Hatam Chaakhorzadeh, for all his help and guidance that has given us over the past two years. Also, the authors would like to express their deep appreciation to Omid Cell and Tissue Center.
References
4. Discussion
Cytokine storm is a lethal systemic inflammatory syndrome defined by hyperactivated immune cells and increased circulating inflammatory cytokines and chemical mediators [19]. It is responsible for the disease severity and mortality in COVID-19 patients [20]. Various studies revealed that severe COVID-19 patients showed higher levels of pro-inflammatory and inflammatory cytokines compared to patients with mild and moderate infections. Hence, early control of the cytokine storm is critical in improving their survival rate [21]. Among the cytokine storm-attenuating therapies, MSC therapy exhibited a promising potential for rapid and significant improvement in clinical symptoms [22].
Due to the immunomodulatory properties of MSCs [23], they attract lots of attention during the pandemic [24-26]. Various studies have evaluated the safety and efficacy of MSCs in severe COVID-19 management (111 clinical trials until October 2022). Also, there are some clinical trials registered on ClinicalTrials data base, applying MSC-derived EVs (NCT05216562, NCT05191381, NCT04798716, NCT04602442, NCT04491240, NCT04493242) or placenta-derived MSCs (NCT04461925, NCT04614025, NCT04389450) in COVID-19. There is just one study (NCT05387278) that evaluated the PMSC-derived EVs in severe COVID-19 conditions, and no data published yet. In agreement with the mentioned clinical trials utilizing MSCs or MSC-derived EVs [27], we detected no intervention-related adverse effects during or after the infusions.
Liu et al. compared severe COVID-19 patients with mild patients and reported a significant and persistent decline in T helper and T cytotoxic lymphocyte counts, contrary to the increase in neutrophils. Therefore, the NLR is a predictive biomarker for COVID-19 outcomes [28]. In agreement with previous studies, NLR results demonstrated a decrease in the intervention group and an increase in the control group. The NLR downtrend through the intervention indicates the treatment’s effectiveness.
CRP is an acute-phase protein that increases in infection or inflammation conditions and serves as a predictive biomarker in COVID-19 patients [29]. Ahnach et al. claimed that CRP level was significantly related to COVID-19 severity [29]. Besides, as CRP indicated the presence of systemic inflammation, Smilowitz et al. suggested that a high level of serum CRP is intensely related to morbidity and mortality in COVID-19 patients [30]. In the present study, CRP decreased in the intervention group and increased in the control group. Hence, the intervention is supposed to be effective in severe COVID-19 patients.
Increased serum creatinine and BUN are independent predictors of severe COVID-19 [31]. Although the increased creatinine level even before the intervention suggested that it was probably due to the COVID-19 infection, the decreased glomerular filtration of EVs and their possible aggregation can also lead to closure and increased creatinine levels.
Fathi-Kazerooni et al. applied MSC-derived Evs from allogeneic menstrual blood in severe COVID-19. Similar to our study, they detected no adverse events following three days of intervention. Also, they reported a significant decrease in CRP after the intervention. Also, consistent with our study, they reported a significant improvement in lymphopenia. Consistently with our findings, they demonstrated that five consecutive doses of MSC-derived secretome improved hypoxia, lessened pulmonary lesions, restored the immune system function, and eased the cytokine storm in severe COVID-19 [32].
Sengupta et al. conducted a cohort study that assessed the safety and efficacy of a single dose of intravenous EVs derived from allogeneic bone marrow MSCs in severe COVID-19. They concluded that EVs from bone marrow MSCs could restore oxygenation, down-regulating cytokine storm, and re-constituting immunity. In accordance with this cohort study, our findings illustrated that applying the MSC-derived EVs can increase SpO2, improve lung injuries, and alleviate cytokine storms [33].
5. Conclusions
Generally, this study demonstrated that intravenous infusion of PMSC-derived EVs decreased cytokine storms, improved pulmonary function, and decreased invasive oxygen/mechanical ventilation support in hospitalized patients with severe COVID-19, with no associated side effects.
Ethical Considerations
Compliance with ethical guidelines
The clinical trial was approved by the Ethics Committee of the Tehran University of Medical Sciences (Code: IR.TUMS.MEDICINE.REC.1399.454).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors would like to thank Hatam Chaakhorzadeh, for all his help and guidance that has given us over the past two years. Also, the authors would like to express their deep appreciation to Omid Cell and Tissue Center.
References
- Gao Z, Xu Y, Sun C, Wang X, Guo Y, Qiu S, et al. A systematic review of asymptomatic infections with COVID-19. Journal of Microbiology, Immunology, and Infection. 2021; 54(1):12-6. [DOI:10.1016/j.jmii.2020.05.001] [PMID]
- Fu L, Wang B, Yuan T, Chen X, Ao Y, Fitzpatrick T, et al. Clinical characteristics of coronavirus disease 2019 (COVID-19) in China: A systematic review and meta-analysis. The Journal of Infection. 2020; 80(6):656-65. [DOI:10.1016/j.jinf.2020.03.041] [PMID]
- Tian W, Jiang W, Yao J, Nicholson CJ, Li RH, Sigurslid HH, et al. Predictors of mortality in hospitalized COVID-19 patients: A systematic review and meta-analysis. Journal of Medical Virology. 2020; 92(10):1875-83. [DOI:10.1002/jmv.26050] [PMID]
- Nikkhah H, Safarzadeh E, Shamsasenjan K, Yousefi M, Lotfinejad P, Talebi M, et al. The effect of bone marrow mesenchymal stem cells on the granulocytic differentiation of HL-60 cells. Turkish Journal of Haematology. 2018; 35(1):42-8. [DOI:10.4274/tjh.2016.0498] [PMID]
- Mazini L, Ezzoubi M, Malka G. Overview of current adipose-derived stem cell (ADSCs) processing involved in therapeutic advancements: Flow chart and regulation updates before and after COVID-19. Stem Cell Research & Therapy. 2021; 12(1):1. [DOI:10.1186/s13287-020-02006-w] [PMID]
- Moradinasab S, Pourbagheri-Sigaroodi A, Zafari P, Ghaffari SH, Bashash D. Mesenchymal stromal/stem cells (MSCs) and MSC-derived extracellular vesicles in COVID-19-induced ARDS: Mechanisms of action, research progress, challenges, and opportunities. International Immunopharmacology. 2021; 97:107694. [DOI:10.1016/j.intimp.2021.107694] [PMID]
- Mohammadian M, Shamsasenjan K, Lotfi Nezhad P, Talebi M, Jahedi M, Nickkhah H, et al. Mesenchymal stem cells: New aspect in cell-based regenerative therapy. Advanced Pharmaceutical Bulletin. 2013; 3(2):433-7. [PMID]
- Coelho A, Alvites RD, Branquinho MV, Guerreiro SG, Maurício AC. Mesenchymal stem cells (MSCs) as a potential therapeutic strategy in COVID-19 patients: Literature research. Frontiers in Cell and Developmental Biology. 2020; 8:602647. [DOI:10.3389/fcell.2020.602647] [PMID]
- Gentile P. SARS-CoV-2: The “Uncensored” truth about its origin and adipose-derived mesenchymal stem cells as new potential immune-modulatory weapon. Aging and Disease. 2021; 12(2):330-44. [DOI:10.14336/AD.2021.0121] [PMID]
- Khanh VC, Fukushige M, Chang YH, Hoang NN, Yamashita T, Obata-Yasuoka M, et al. Wharton’s jelly mesenchymal stem cell-derived extracellular vesicles reduce sars-cov2-induced inflammatory cytokines under high glucose and uremic toxin conditions. Stem Cells and Development. 2021; 30(15):758-72. [DOI:10.1089/scd.2021.0065] [PMID]
- Shi MM, Yang QY, Monsel A, Yan JY, Dai CX, Zhao JY, et al. Preclinical efficacy and clinical safety of clinical‐grade nebulized allogenic adipose mesenchymal stromal cells‐derived extracellular vesicles. Journal of Extracellular Vesicles. 2021; 10(10):e12134. [DOI:10.1002/jev2.12134] [PMID]
- da Silva KN, Gobatto ALN, Costa-Ferro ZSM, Cavalcante BRR, Caria ACI, de Aragão França LS, et al. Is there a place for mesenchymal stromal cell-based therapies in the therapeutic armamentarium against COVID-19? Stem Cell Research & Therapy. 2021; 12(1):425. [DOI:10.1186/s13287-021-02502-7] [PMID]
- Yan YY, Zhou WM, Wang YQ, Guo QR, Zhao FX, Zhu ZY, et al. The potential role of extracellular vesicles in COVID-19 treatment: Opportunity and challenge. Frontiers in Molecular Biosciences. 2021; 8:699929. [DOI:10.3389/fmolb.2021.699929] [PMID]
- Kim H, Lee MJ, Bae EH, Ryu JS, Kaur G, Kim HJ, et al. Comprehensive molecular profiles of functionally effective MSC-derived extracellular vesicles in immunomodulation. Molecular Therapy. 2020; 28(7):1628-44. [DOI:10.1016/j.ymthe.2020.04.020] [PMID]
- Yousefi Dehbidi M, Goodarzi N, Azhdari MH, Doroudian M. Mesenchymal stem cells and their derived exosomes to combat Covid-19. Reviews in Medical Virology. 2022; 32(2):e2281. [PMID]
- Panda B, Sharma Y, Gupta S, Mohanty S. Mesenchymal stem cell-derived exosomes as an emerging paradigm for regenerative therapy and nano-medicine: A comprehensive review. Life. 2021; 11(8):784. [DOI:10.3390/life11080784] [PMID]
- Hashemian SR, Aliannejad R, Zarrabi M, Soleimani M, Vosough M, Hosseini SE, et al. Mesenchymal stem cells derived from perinatal tissues for treatment of critically ill COVID-19-induced ARDS patients: A case series. Stem Cell Research & Therapy. 2021; 12(1):91. [DOI:10.1186/s13287-021-02165-4] [PMID]
- Wiklander OP, Bostancioglu RB, Welsh JA, Zickler AM, Murke F, Corso G, et al. Systematic methodological evaluation of a multiplex bead-based flow cytometry assay for detection of extracellular vesicle surface signatures. Frontiers in Immunology. 2018; 9:1326. [DOI:10.3389/fimmu.2018.01326] [PMID]
- Fajgenbaum DC, June CH. Cytokine storm. The New England Journal of Medicine. 2020; 383(23):2255-73. [DOI:10.1056/NEJMra2026131] [PMID]
- Mehta P, McAuley DF, Brown M, Sanchez E, Tattersall RS, Manson JJ, et al. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet. 2020; 395(10229):1033-4. [DOI:10.1016/S0140-6736(20)30628-0] [PMID]
- Hu B, Huang S, Yin L. The cytokine storm and COVID-19. Journal of Medical Virology. 2021; 93(1):250-6. [DOI:10.1002/jmv.26232] [PMID]
- Metcalfe SM. Mesenchymal stem cells and management of COVID-19 pneumonia. Medicine in Drug Discovery. 2020; 5:100019. [DOI:10.1016/j.medidd.2020.100019] [PMID]
- Mohammadian M, Abasi E, Akbarzadeh A. Mesenchymal stem cell-based gene therapy: A promising therapeutic strategy. Artificial Cells, Nanomedicine, and Biotechnology. 2016; 44(5):1206-11. [DOI:10.3109/21691401.2015.1029624] [PMID]
- Feng G, Shi L, Huang T, Ji N, Zheng Y, Lin H, et al. Human umbilical cord mesenchymal stromal cell treatment of severe COVID-19 patients: A 3-month follow-up study following hospital discharge. Stem Cells and Development. 2021; 30(15):773-81. [DOI:10.1089/scd.2021.0015] [PMID]
- Leng Z, Zhu R, Hou W, Feng Y, Yang Y, Han Q, et al. Transplantation of ACE2-mesenchymal stem cells improves the outcome of patients with COVID-19 pneumonia. Aging and Disease. 2020; 11(2):216-28. [DOI:10.14336/AD.2020.0228] [PMID]
- Xu X, Jiang W, Chen L, Xu Z, Zhang Q, Zhu M, et al. Evaluation of the safety and efficacy of using human menstrual blood-derived mesenchymal stromal cells in treating severe and critically ill COVID-19 patients: An exploratory clinical trial. Clinical and Translational Medicine. 2021; 11(2):e297. [DOI:10.1002/ctm2.297] [PMID]
- Abdelgawad M, Bakry NS, Farghali AA, Abdel-Latif A, Lotfy A. Mesenchymal stem cell-based therapy and exosomes in COVID-19: Current trends and prospects. Stem Cell Research & Therapy. 2021; 12(1):469. [DOI:10.1186/s13287-021-02542-z] [PMID]
- Liu J, Li S, Liu J, Liang B, Wang X, Wang H, et al. Longitudinal characteristics of lymphocyte responses and cytokine profiles in the peripheral blood of SARS-CoV-2 infected patients. EBioMedicine. 2020; 55:102763. [DOI:10.1016/j.ebiom.2020.102763] [PMID]
- Ahnach M, Zbiri S, Nejjari S, Ousti F, Elkettani C. C-reactive protein as an early predictor of COVID-19 severity. Journal of Medical Biochemistry. 2020; 39(4):500-7. [DOI:10.5937/jomb0-27554] [PMID]
- Smilowitz NR, Kunichoff D, Garshick M, Shah B, Pillinger M, Hochman JS, et al. C-reactive protein and clinical outcomes in patients with COVID-19. European Heart Journal, 2021; 42(23):2270-9. [DOI:10.1093/eurheartj/ehaa1103] [PMID]
- Ok F, Erdogan O, Durmus E, Carkci S, Canik A. Predictive values of blood urea nitrogen/creatinine ratio and other routine blood parameters on disease severity and survival of COVID‐19 patients. Journal of Medical Virology. 2021; 93(2):786-93. [DOI:10.1002/jmv.26300] [PMID]
- Fathi-Kazerooni M, Fattah-Ghazi S, Darzi M, Makarem J, Nasiri R, Salahshour F, et al. Safety and efficacy study of allogeneic human menstrual blood stromal cells secretome to treat severe COVID-19 patients: Clinical trial phase I & II. Stem Cell Research & Therapy. 2022; 13(1):96. [DOI:10.1186/s13287-022-02771-w] [PMID]
- Sengupta V, Sengupta S, Lazo A, Woods P, Nolan A, Bremer N. Exosomes derived from bone marrow mesenchymal stem cells as treatment for severe COVID-19. Stem Cells and Development. 2020; 29(12):747-54. [DOI:10.1089/scd.2020.0080] [PMID]
Type of Study: Original |
Subject:
Stem Cell
Received: 2022/10/18 | Accepted: 2022/11/13 | Published: 2022/07/1
Received: 2022/10/18 | Accepted: 2022/11/13 | Published: 2022/07/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Anatomical Sciences Journal (ASJ)
Negah Institute for Scientific Communication, No.15, Na'eemi St., Mirzaye Shirazi St., Tehran, Iran.
Publisher Tel : +9821 4535 5555;
+9821 4535 5000
Website: http://www.anatomyjournal.ir/
E-mail: anatomyjournal@gmail.com
