Sun, Jul 26, 2026
Volume 19, Issue 2 (Summer & Autumn 2022)
ASJ 2022, 19(2): 65-72 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hlongwane H, Pillay-Addinal S, Govender-Davies S. A Clinical Evaluation of the Length of Segments and Branches of the Brachial Plexus. ASJ 2022; 19 (2) :65-72
URL: http://anatomyjournal.ir/article-1-569-en.html
URL: http://anatomyjournal.ir/article-1-569-en.html



1- Department of Anatomy and Histology, School of Medicine, Sefako Makgatho Health Sciences University, Ga-Rankuwa, South Africa.
Full-Text [PDF 2570 kb]
(587 Downloads)
| Abstract (HTML) (2855 Views)
Full-Text: (1325 Views)
1. Introduction
The brachial plexus (BP) is a network of nerves originating in the periclavicular region and provides sensory and motor innervation to the upper extremity. The plexus is an important structure due to its anatomical location and vulnerability to damage [1]. Therefore, BP injuries are common and can result from accidental, traumatic, or surgical incidences [2]. As such, surgeons need to be able to locate individual plexus segments or nerve branches when performing procedures. However, it can prove challenging to identify the :union: and dividing sites of nerves within the BP [3]. There is considerable diversity of opinion regarding the anatomical landmarks for the BP. The supraclavicular triangle or pectoralis minor muscle is commonly used as a reference point [4]. However, these landmarks do not predict the branching pattern of nerves within the plexus. Therefore, it is essential to map the segmentation and branching patterns of individual nerves within the BP, as this can lead to the successful management of regional anesthesia and positive outcomes from surgical intervention.
The primary aim of this study was to determine the average length of individual segments and nerve branches within the BP. The secondary purpose was to provide insight into the anatomical landmarks and variations that may occur within the BP in the periclavicular area. To our knowledge, this is one of a few studies that examined the length of the BP segments and nerve branches.
2. Material and Methods
Once approval was obtained, thirty formalin-fixed adult cadavers (24 males and 6 females) were used in this study. All cadaveric material was handled in accordance with the South African National Health Act, 61 of 2003. Demographic information was recorded and kept confidential. The cadavers ranged from 28 to 83 years of age. To expose the BP, cadavers were placed in a supine position, with the arm abducted for greater access to the axilla region. Several skin incisions were done bilaterally (n=60) from the anterior tubercle of the cervical transverse process to the distal aspect of the hand. Dissections were performed from superficial to deep using a standard dissection kit to ensure the removal of structures while noting the anatomical landmarks. After skin incisions, the platysma, sternocleidomastoid, pectoralis (both major and minor), and anterior and middle scalene muscles were reflected at their insertion sites, while the clavicle was removed. The terminal branches of the BP were further dissected to expose their course within the anterior and posterior compartments of the arm, forearm, and hand.
The following measurements were taken using a sliding dial caliper: 1. The length of the roots from the cervical (and thoracic) transverse process (the first tangible landmark) to the uniting point of the superior and inferior trunk (and continuation point of the middle trunk), 2. The length of the trunks from the point of unity to the point of division, 3. The size of the divisions from the point of division to the point of uniting (continuation), 4. The length of the cords from their point of unity to the point of division, 5. The size of the individual terminal branches (musculocutaneous, median, ulnar, radial, and axillary nerves) from their point of division along their course towards an end target structure (Figure 1).
 Upon inspection of the course of the terminal branches–specifically the median, radial, and ulnar nerves, most branches were cut or damaged in the forearm region. Therefore, to keep measurements consistent, the median, radial, and ulnar nerves were measured until their entry/course through the cubital fossa before the nerves gave off branches or further divided into terminal branches. The musculocutaneous nerve was measured to its endpoint as it pierced the coracobrachialis muscle, and the axillary nerve was measured at its endpoint, which was its entry into the triangular interval.
Upon inspection of the course of the terminal branches–specifically the median, radial, and ulnar nerves, most branches were cut or damaged in the forearm region. Therefore, to keep measurements consistent, the median, radial, and ulnar nerves were measured until their entry/course through the cubital fossa before the nerves gave off branches or further divided into terminal branches. The musculocutaneous nerve was measured to its endpoint as it pierced the coracobrachialis muscle, and the axillary nerve was measured at its endpoint, which was its entry into the triangular interval.
Photographs that included a scale were taken of each sample (Figure 2).
 Images were then uploaded onto ImageJ softeware, version 1.53t (year 2022, 64-bit, Java 8) to confirm the measurements taken. Additionally, any variations found within the BP were noted and recorded. Anatomical landmarks related to the segments and branches of the BP were noted throughout its entire course.
Images were then uploaded onto ImageJ softeware, version 1.53t (year 2022, 64-bit, Java 8) to confirm the measurements taken. Additionally, any variations found within the BP were noted and recorded. Anatomical landmarks related to the segments and branches of the BP were noted throughout its entire course.
Statistical analysis
All measurements taken were inputted into a Microsoft Excel spreadsheet. Statistical analyses included descriptive statistics, Mean±SD, and the minimum and maximum values of measurements. Inter-rater and intra-rater methods were used to further confirm validity and accuracy. The principal investor completed all measurements twice, first by using cotton and a sliding dial caliper and secondly by using image J to confirm measurements from the photographs. A secondary investigator completed 25% of the measurements which were further tested for accuracy using a student t-test. After testing the data for normality, comparisons between the left- and right-hand sides were done using a paired t-test. If the data was not statistically significant, the data were then pooled together to create a list of means with new standard deviations.
3. Results
Measurements
All statistical analysis was performed using SPSS , version 26. Results revealed the data to be normally distributed. Subsequently, paired t-tests were performed for left- and right-hand side measurements. Normality was further confirmed as the mean for each measurement was twice the standard deviation. Overall, there were 11 comparisons, due to which the Bonferroni correction method was adopted. This correction method is used to alter the P when numerous dependent or independent statistical tests are being performed simultaneously on a single data set. The Bonferroni correction method decreases the chances of obtaining type I errors when multiple paired tests are performed on a single data set. The test is done by dividing the critical P (α/alpha) by the number of comparisons made. For this study, it was 0.05/11=0.0045. Therefore, significance was determined by a P<0.0045. Table 1 summarizes the results from the paired t-tests.

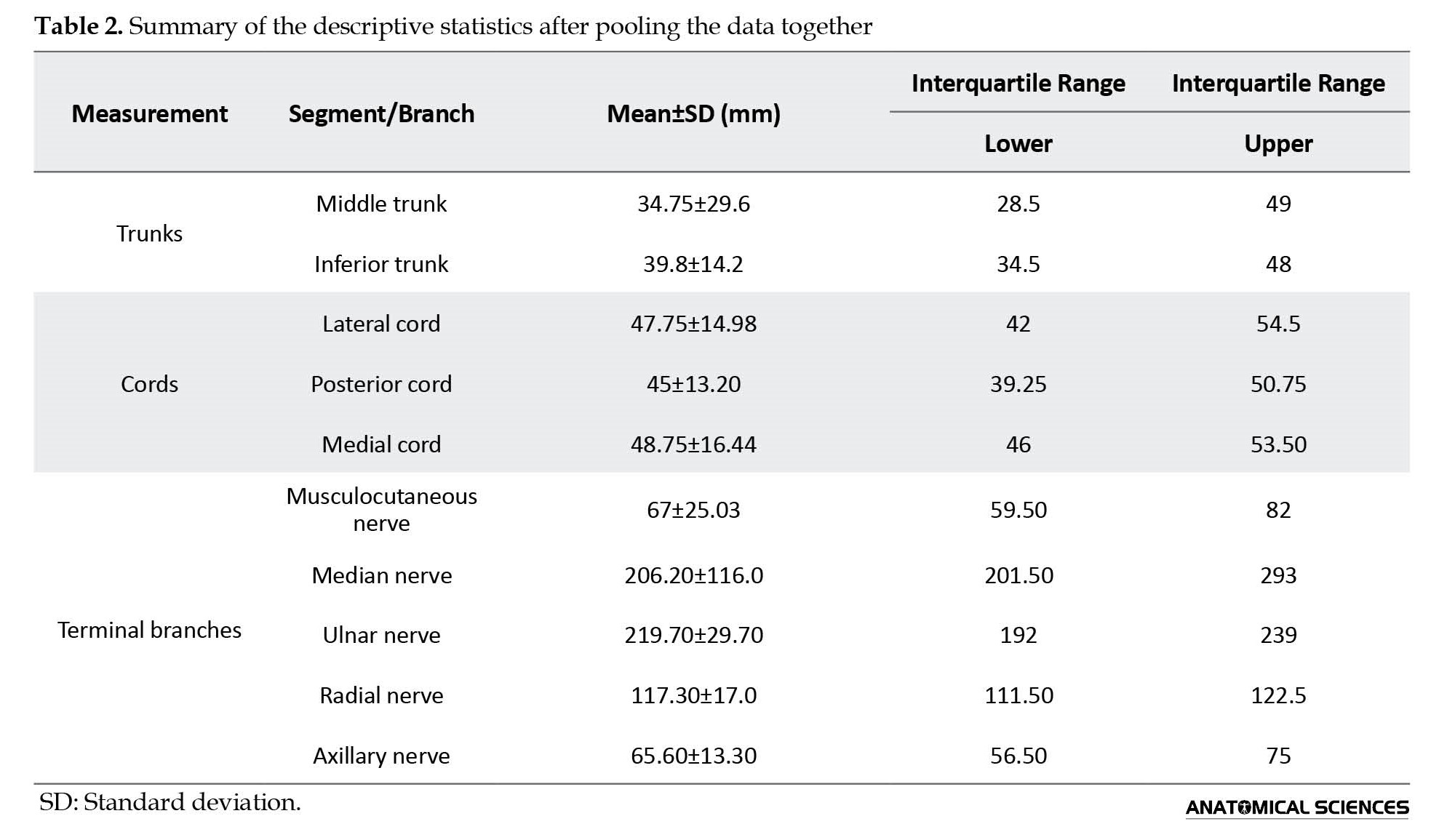
Results from the paired t-test displayed a statistical significance between left- and right-hand sides for the superior trunk as the P<0.0045 (confidence interval of 95%). Measurements that weren’t statistically significant were then pooled together to create means for each measurement with a new standard deviation (Table 2).
Anatomy
Upon dissection of the BP segments and branches, the plexus roots were found to be damaged in most samples. Therefore, only variations (rather than measurements) in the plexus roots were noted. All BPs were found between the anterior and middle scalene muscles. From the total sample size (n=60), 90% of the sample displayed normal anatomy, while the remaining 10% displayed abnormal variants. In 5% (n=3) of cases, the median nerve was seen splitting into the individual nerve roots (lateral and median) before entering the forearm compartment. In 3.3% (n=2) of the cases, the axillary nerve gave off anterior and posterior branches before entering the quadrangular space. Lastly, in 1.7% (n=1), the median nerve gave off multiple secondary (muscular) branches before entering the forearm. Moreover, the BP was evaluated for pre and post-fixtures. Results revealed that 30% of the sample had a pre-fixed BP, while 10% was post-fixed. The remaining cadavers were normally fixed (60%).
4. Discussion
Variations of the BP and its terminal branches are not uncommon and have been thoroughly documented [5]. Therefore, it is essential to understand the complex anatomical structure of the BP to be able to apply surgical procedures to both normal and variant BPs. Furthermore, anatomical landmarks, variations, and segmental distances are useful in a clinical setting to help reduce the risk of complications or the number of failed regional nerve blocks. This study aimed to determine the average length of individual segments and branches of the BP. Results from this study revealed no significant difference between the left- and right-hand sides. The BP segments and branches were easy to identify and follow along their course towards their terminal destination. To our knowledge, this is only one study that reported on the distances of the parts of the BP (Table 2).
In a study conducted in Iran, the BP of 32 fresh none embalmed cadavers were evaluated. The cadavers were dissected bilaterally to measure the terminal branches of the BP. Results from the study reveal the mean length for the terminal branches to be as follows: The axillary nerve 3.9±0.5 cm (confidence interval 3.7–4.1), the radial nerve 7.6±1.3 cm (confidence interval 7.2–8.1), the ulnar nerve 56.3±2.7 cm (confidence interval 55.5–57.2), the musculocutaneous nerve 12.6±2.2 cm (confidence interval 12.1–13.1) and the median nerve 58.5±7.4 cm (confidence interval 57–60) [6]. Compared to the current study, the length of the axillary nerve was similar. However, the size of the musculocutaneous nerve was half of that found in Emamhadi et al.’s study [6]. Discrepancies in the musculocutaneous distance could result from diverse measuring points, as the start and endpoints were not specified. Additionally, the radial, ulnar, and median nerves were almost double the distance compared to the current study. However, the endpoint of these nerves was at the cubital fossa, whereas, in Emamhadi et al.’s., study the endpoints of the nerves were followed towards the terminal muscles in the forearm.
Lee et al. conducted a study to determine the normal morphometric landmarks of the uniting and dividing points of the BP. Using 10 adult cadavers, the BP was exposed to allow for various measurements above and below the clavicle [3]. Results from the supraclavicular region revealed the distance from the chassaignac tubercle to the uniting point of the superior trunk (the root of the BP) was 21±7 mm. The distance from the Chassaignac tubercle to the dividing point of the superior trunk was 42±5 mm. The distance from the chassaignac tubercle to the dividing point of the middle trunk was similar to the superior trunk, 43±10 mm. Additionally, the average distance from the superior border of the clavicle to the uniting point of the superior trunk was 44±11 mm, while the distance to the dividing point of the superior trunk was 19±4 mm. Results from the infraclavicular region revealed the distance from the inferior border of the clavicle to the uniting point of the lateral cord was 1.5±8 mm. The distance from the inferior border of the clavicle to the exit point of the musculocutaneous nerve was 49±12 mm. The distance from the inferior border of the clavicle to the uniting point of the median nerve was 57±7 mm. The distance from the inferior border of the clavicle to the uniting point of the ulnar nerve was 3.3±10 mm. In most cases, the musculocutaneous nerve exited at a point 22 mm distal to the lateral margin of the pectoralis minor muscle rather than 16 mm proximal to the lateral margin of the muscle [3]. Results from Lee et al.’s., study are different from the current study as they focused on the clavicle being the main point of reference when taking measurements. Furthermore, they only reported on parts of the BP, not the entire BP.
In another study, the length of the branches of BP was measured in an adult cadaveric sample. The authors reported that, on average, the uniting points of the trunks from the intervertebral foramen were 43 mm from the spinal root C5, 50 mm from spinal root C6, and 58 mm from the spinal root C7. The average length of the lateral cord was 60 mm, while the average length of the medial cord was 50 mm [7]. Compared to the current study, the average length of the lateral cord was shorter, 48 mm (ranging from 42 to 55 mm). The average length of the medial cord was comparable (49 mm).
In a study conducted by Zhong et al., the detailed microanatomy of the BP roots was explored to provide an anatomical basis for BP injuries. The authors used the cervical and thoracic region of 15 adult anticorrosive cadaveric samples. Results revealed the origin of the anterior nerve roots in the dorsal to a ventral direction to be a minimum of 2.2 mm at C5, while the maximum was 3.1 mm at T1. The posterior nerve root was a maximum of 4.2 mm at C5, yet a minimum of 2.7 mm T1. Additionally, the authors recorded the angle between the anterior and posterior nerve roots. The angle between the anterior root and spinal cord gradually decreased from 51.4⁰ at C5 to 21.7⁰ at T1. Likewise, there was a gradual decrease in the angle of the posterior roots from 54.8⁰ at C5 to 19.9⁰ at T1. The authors concluded their study, by stating that nerve roots C7-8 and T1 of the BP were more prone to injury when compared to nerve roots C5-6 [8].
In a recent study, the origin of the anterior and posterior divisions of the BP with their respective trunks, as well as the positions of the cords of the BP were examined. Results revealed the posterior divisions had a cranial and dorsal origin, while the anterior divisions had a caudal and ventral origin. Regarding the position of the cords, the posterior cord was most cranial, while the lateral cord was central and the medial cord was most caudal. Additionally, they found the posterior division of the superior trunk to be between the suprascapular nerve and its anterior division. The authors concluded that the BP diagrams in most articles differ in terms of the arrangement of the posterior division of the superior trunk [9].
Although the BP is formed from spinal roots C5 to T1, it can receive contributions from C4 and T2. If it receives contributions from spinal root C4, the BP will be formed from spinal roots C4 to C7 and is described as being pre-fixed. However, if it receives contributions from spinal root T2, the BP will be formed from spinal roots C6 to T2 and is described as being post-fixed. In the current study, 30% of the sample was found to be pre-fixed, while 10% was post-fixed. These results were much higher than previous studies, which reported an average of 22% / 9.4% pre-fixed [6, 10] and 1% / 3.1% post-fixed [11, 6]. In a cadaveric fetal study, the BP was normally formed with contributions from both spinal roots C4 and T2 in all cases [1]. In a more recent study, the BP was found to have four trunks, with contributions from both the C4 and T2 in 5% of the study [12].
Throughout the dissections, anatomical landmarks were noted for the various segments of the BP. The anterior rami of the spinal nerve roots of the BP exit at the intervertebral foramen. The roots then travel in-between the anterior and middle scalene muscles via the sulcus nervi spinalis of the transverse process at grade as described by Lee et al. [3]. In the majority of our cadavers, the superior and middle trunks were noted to form at the anterolateral border of the middle scalene muscle. While the inferior trunk formed at the medial margin of the first rib. The trunks then were divided into their anterior and posterior divisions in the supraclavicular fossa at the level of the 1st rib. Regarding the subclavian artery, the superior and middle trunks were found anterolateral to the artery, while the inferior trunk was located posterior to the artery. The divisions then united into the cords positioned around the axillary artery. The lateral cord was found lateral to one-third of the axillary artery, while the medial cord was found medial to the same one-third of the axillary artery. The posterior cord was located posterior to one-third of the artery.
Subsequently, the anatomical landmarks related to the course of each of the terminal branches were also noted. The musculocutaneous nerve, which is the lateral cord’s terminal branch, originates/emerges at the inferolateral border of the pectoralis minor muscle. The nerve then pierced the coracobrachialis muscle (lower half of the muscle) to travel inferiorly between the biceps brachii and brachioradialis muscles. Proximal to the cubital fossa, the nerve continued into the forearm as the lateral cutaneous nerve. The axillary nerve branched off the posterior cord to travel posteriorly through the quadrangular space to enter into the posterior compartment of the arm. It then travels inferolateral on the subscapularis muscle to further split into anterior and posterior branches. The radial nerve (terminal branch of the posterior cord) travels posteriorly through the triangular interval to enter the arm’s posterior compartment. Once there, the nerve traveled inferiorly in the radial groove towards the lateral epicondyle. It then entered the cubital fossa anterior to the lateral epicondyle to terminate into its superficial sensory and deep motor branches.
The median nerve traveled inferiorly down the arm, anterior to the axillary artery, and lateral to the brachial artery. At the origin of the brachioradialis muscle, the median nerve crossed over the brachial artery to lie medial to the artery while entering the cubital fossa. Then, the nerve traveled through the flexor digitorum profundus and flexor digitorum superficialis muscles in the forearm while giving off two major branches. It then traveled through the carpal tunnel to enter the hand before terminating into two branches. Lastly, the ulnar nerve descended the arm, between the axillary artery and vein. Midway down the artery, the nerve shifted to lie medial to the brachial artery. It then pierced the fascial septum to enter the posterior compartment of the arm to travel posterior to the medial epicondyle to enter the forearm. In the forearm, the nerve traveled deep to the flexor carpi ulnaris towards the wrist joint. At the joint, the nerve was found superficial to the flexor retinaculum of the hand and medial to the ulnar artery while entering the hand.
5. Conclusion
A thorough understanding of all relevant anatomical landmarks is mandatory for any successful procedure. Common techniques such as BP blocks require detailed anatomical literature due to the complexity and variability of the plexus. The mean length of the trunks was 37.3±2.5 mm, and the cords 47±1.8 mm. The mean length of the terminal branches ranged from 65 to 220 mm. Results from this study will add to the understanding of the anatomy of the BP and further assist clinicians in pre- and perioperative surgical planning.
Limitations and recommendation
A major limitation of this study was the sample size. Therefore, we recommend future studies with a larger sample size together with the aid of imagining modalities such as ultrasound guidance to fully evaluate the anatomy of the BP. Additionally, as this was a retrospective investigation using already embalmed cadavers, tissue shrinkage may influence the measurements.
Ethical Considerations
Compliance with ethical guidelines
Ethical approval was obtained from the Sefako Makgatho Health Sciences University, Research Ethics Committee (SMUREC) (Code: SMUREC/M/165/2020:PG).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and study design: Hazel Hlongwan and Govender-Davies; Data acquisition: Hazel Hlongwan and Sashrika Pillay-Addinal; Data analysis and data interpretation: Hazel Hlongwan; Revising the manuscript for critically for important intellectual content: Sashrika Pillay-Addinal and Sabashnee Govender-Davies; Drafting the article, and final approval: Sabashnee Govender-Davies.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank everyone who was involved in conducting this research.
References
The brachial plexus (BP) is a network of nerves originating in the periclavicular region and provides sensory and motor innervation to the upper extremity. The plexus is an important structure due to its anatomical location and vulnerability to damage [1]. Therefore, BP injuries are common and can result from accidental, traumatic, or surgical incidences [2]. As such, surgeons need to be able to locate individual plexus segments or nerve branches when performing procedures. However, it can prove challenging to identify the :union: and dividing sites of nerves within the BP [3]. There is considerable diversity of opinion regarding the anatomical landmarks for the BP. The supraclavicular triangle or pectoralis minor muscle is commonly used as a reference point [4]. However, these landmarks do not predict the branching pattern of nerves within the plexus. Therefore, it is essential to map the segmentation and branching patterns of individual nerves within the BP, as this can lead to the successful management of regional anesthesia and positive outcomes from surgical intervention.
The primary aim of this study was to determine the average length of individual segments and nerve branches within the BP. The secondary purpose was to provide insight into the anatomical landmarks and variations that may occur within the BP in the periclavicular area. To our knowledge, this is one of a few studies that examined the length of the BP segments and nerve branches.
2. Material and Methods
Once approval was obtained, thirty formalin-fixed adult cadavers (24 males and 6 females) were used in this study. All cadaveric material was handled in accordance with the South African National Health Act, 61 of 2003. Demographic information was recorded and kept confidential. The cadavers ranged from 28 to 83 years of age. To expose the BP, cadavers were placed in a supine position, with the arm abducted for greater access to the axilla region. Several skin incisions were done bilaterally (n=60) from the anterior tubercle of the cervical transverse process to the distal aspect of the hand. Dissections were performed from superficial to deep using a standard dissection kit to ensure the removal of structures while noting the anatomical landmarks. After skin incisions, the platysma, sternocleidomastoid, pectoralis (both major and minor), and anterior and middle scalene muscles were reflected at their insertion sites, while the clavicle was removed. The terminal branches of the BP were further dissected to expose their course within the anterior and posterior compartments of the arm, forearm, and hand.
The following measurements were taken using a sliding dial caliper: 1. The length of the roots from the cervical (and thoracic) transverse process (the first tangible landmark) to the uniting point of the superior and inferior trunk (and continuation point of the middle trunk), 2. The length of the trunks from the point of unity to the point of division, 3. The size of the divisions from the point of division to the point of uniting (continuation), 4. The length of the cords from their point of unity to the point of division, 5. The size of the individual terminal branches (musculocutaneous, median, ulnar, radial, and axillary nerves) from their point of division along their course towards an end target structure (Figure 1).
Photographs that included a scale were taken of each sample (Figure 2).
Statistical analysis
All measurements taken were inputted into a Microsoft Excel spreadsheet. Statistical analyses included descriptive statistics, Mean±SD, and the minimum and maximum values of measurements. Inter-rater and intra-rater methods were used to further confirm validity and accuracy. The principal investor completed all measurements twice, first by using cotton and a sliding dial caliper and secondly by using image J to confirm measurements from the photographs. A secondary investigator completed 25% of the measurements which were further tested for accuracy using a student t-test. After testing the data for normality, comparisons between the left- and right-hand sides were done using a paired t-test. If the data was not statistically significant, the data were then pooled together to create a list of means with new standard deviations.
3. Results
Measurements
All statistical analysis was performed using SPSS , version 26. Results revealed the data to be normally distributed. Subsequently, paired t-tests were performed for left- and right-hand side measurements. Normality was further confirmed as the mean for each measurement was twice the standard deviation. Overall, there were 11 comparisons, due to which the Bonferroni correction method was adopted. This correction method is used to alter the P when numerous dependent or independent statistical tests are being performed simultaneously on a single data set. The Bonferroni correction method decreases the chances of obtaining type I errors when multiple paired tests are performed on a single data set. The test is done by dividing the critical P (α/alpha) by the number of comparisons made. For this study, it was 0.05/11=0.0045. Therefore, significance was determined by a P<0.0045. Table 1 summarizes the results from the paired t-tests.
Results from the paired t-test displayed a statistical significance between left- and right-hand sides for the superior trunk as the P<0.0045 (confidence interval of 95%). Measurements that weren’t statistically significant were then pooled together to create means for each measurement with a new standard deviation (Table 2).
Anatomy
Upon dissection of the BP segments and branches, the plexus roots were found to be damaged in most samples. Therefore, only variations (rather than measurements) in the plexus roots were noted. All BPs were found between the anterior and middle scalene muscles. From the total sample size (n=60), 90% of the sample displayed normal anatomy, while the remaining 10% displayed abnormal variants. In 5% (n=3) of cases, the median nerve was seen splitting into the individual nerve roots (lateral and median) before entering the forearm compartment. In 3.3% (n=2) of the cases, the axillary nerve gave off anterior and posterior branches before entering the quadrangular space. Lastly, in 1.7% (n=1), the median nerve gave off multiple secondary (muscular) branches before entering the forearm. Moreover, the BP was evaluated for pre and post-fixtures. Results revealed that 30% of the sample had a pre-fixed BP, while 10% was post-fixed. The remaining cadavers were normally fixed (60%).
4. Discussion
Variations of the BP and its terminal branches are not uncommon and have been thoroughly documented [5]. Therefore, it is essential to understand the complex anatomical structure of the BP to be able to apply surgical procedures to both normal and variant BPs. Furthermore, anatomical landmarks, variations, and segmental distances are useful in a clinical setting to help reduce the risk of complications or the number of failed regional nerve blocks. This study aimed to determine the average length of individual segments and branches of the BP. Results from this study revealed no significant difference between the left- and right-hand sides. The BP segments and branches were easy to identify and follow along their course towards their terminal destination. To our knowledge, this is only one study that reported on the distances of the parts of the BP (Table 2).
In a study conducted in Iran, the BP of 32 fresh none embalmed cadavers were evaluated. The cadavers were dissected bilaterally to measure the terminal branches of the BP. Results from the study reveal the mean length for the terminal branches to be as follows: The axillary nerve 3.9±0.5 cm (confidence interval 3.7–4.1), the radial nerve 7.6±1.3 cm (confidence interval 7.2–8.1), the ulnar nerve 56.3±2.7 cm (confidence interval 55.5–57.2), the musculocutaneous nerve 12.6±2.2 cm (confidence interval 12.1–13.1) and the median nerve 58.5±7.4 cm (confidence interval 57–60) [6]. Compared to the current study, the length of the axillary nerve was similar. However, the size of the musculocutaneous nerve was half of that found in Emamhadi et al.’s study [6]. Discrepancies in the musculocutaneous distance could result from diverse measuring points, as the start and endpoints were not specified. Additionally, the radial, ulnar, and median nerves were almost double the distance compared to the current study. However, the endpoint of these nerves was at the cubital fossa, whereas, in Emamhadi et al.’s., study the endpoints of the nerves were followed towards the terminal muscles in the forearm.
Lee et al. conducted a study to determine the normal morphometric landmarks of the uniting and dividing points of the BP. Using 10 adult cadavers, the BP was exposed to allow for various measurements above and below the clavicle [3]. Results from the supraclavicular region revealed the distance from the chassaignac tubercle to the uniting point of the superior trunk (the root of the BP) was 21±7 mm. The distance from the Chassaignac tubercle to the dividing point of the superior trunk was 42±5 mm. The distance from the chassaignac tubercle to the dividing point of the middle trunk was similar to the superior trunk, 43±10 mm. Additionally, the average distance from the superior border of the clavicle to the uniting point of the superior trunk was 44±11 mm, while the distance to the dividing point of the superior trunk was 19±4 mm. Results from the infraclavicular region revealed the distance from the inferior border of the clavicle to the uniting point of the lateral cord was 1.5±8 mm. The distance from the inferior border of the clavicle to the exit point of the musculocutaneous nerve was 49±12 mm. The distance from the inferior border of the clavicle to the uniting point of the median nerve was 57±7 mm. The distance from the inferior border of the clavicle to the uniting point of the ulnar nerve was 3.3±10 mm. In most cases, the musculocutaneous nerve exited at a point 22 mm distal to the lateral margin of the pectoralis minor muscle rather than 16 mm proximal to the lateral margin of the muscle [3]. Results from Lee et al.’s., study are different from the current study as they focused on the clavicle being the main point of reference when taking measurements. Furthermore, they only reported on parts of the BP, not the entire BP.
In another study, the length of the branches of BP was measured in an adult cadaveric sample. The authors reported that, on average, the uniting points of the trunks from the intervertebral foramen were 43 mm from the spinal root C5, 50 mm from spinal root C6, and 58 mm from the spinal root C7. The average length of the lateral cord was 60 mm, while the average length of the medial cord was 50 mm [7]. Compared to the current study, the average length of the lateral cord was shorter, 48 mm (ranging from 42 to 55 mm). The average length of the medial cord was comparable (49 mm).
In a study conducted by Zhong et al., the detailed microanatomy of the BP roots was explored to provide an anatomical basis for BP injuries. The authors used the cervical and thoracic region of 15 adult anticorrosive cadaveric samples. Results revealed the origin of the anterior nerve roots in the dorsal to a ventral direction to be a minimum of 2.2 mm at C5, while the maximum was 3.1 mm at T1. The posterior nerve root was a maximum of 4.2 mm at C5, yet a minimum of 2.7 mm T1. Additionally, the authors recorded the angle between the anterior and posterior nerve roots. The angle between the anterior root and spinal cord gradually decreased from 51.4⁰ at C5 to 21.7⁰ at T1. Likewise, there was a gradual decrease in the angle of the posterior roots from 54.8⁰ at C5 to 19.9⁰ at T1. The authors concluded their study, by stating that nerve roots C7-8 and T1 of the BP were more prone to injury when compared to nerve roots C5-6 [8].
In a recent study, the origin of the anterior and posterior divisions of the BP with their respective trunks, as well as the positions of the cords of the BP were examined. Results revealed the posterior divisions had a cranial and dorsal origin, while the anterior divisions had a caudal and ventral origin. Regarding the position of the cords, the posterior cord was most cranial, while the lateral cord was central and the medial cord was most caudal. Additionally, they found the posterior division of the superior trunk to be between the suprascapular nerve and its anterior division. The authors concluded that the BP diagrams in most articles differ in terms of the arrangement of the posterior division of the superior trunk [9].
Although the BP is formed from spinal roots C5 to T1, it can receive contributions from C4 and T2. If it receives contributions from spinal root C4, the BP will be formed from spinal roots C4 to C7 and is described as being pre-fixed. However, if it receives contributions from spinal root T2, the BP will be formed from spinal roots C6 to T2 and is described as being post-fixed. In the current study, 30% of the sample was found to be pre-fixed, while 10% was post-fixed. These results were much higher than previous studies, which reported an average of 22% / 9.4% pre-fixed [6, 10] and 1% / 3.1% post-fixed [11, 6]. In a cadaveric fetal study, the BP was normally formed with contributions from both spinal roots C4 and T2 in all cases [1]. In a more recent study, the BP was found to have four trunks, with contributions from both the C4 and T2 in 5% of the study [12].
Throughout the dissections, anatomical landmarks were noted for the various segments of the BP. The anterior rami of the spinal nerve roots of the BP exit at the intervertebral foramen. The roots then travel in-between the anterior and middle scalene muscles via the sulcus nervi spinalis of the transverse process at grade as described by Lee et al. [3]. In the majority of our cadavers, the superior and middle trunks were noted to form at the anterolateral border of the middle scalene muscle. While the inferior trunk formed at the medial margin of the first rib. The trunks then were divided into their anterior and posterior divisions in the supraclavicular fossa at the level of the 1st rib. Regarding the subclavian artery, the superior and middle trunks were found anterolateral to the artery, while the inferior trunk was located posterior to the artery. The divisions then united into the cords positioned around the axillary artery. The lateral cord was found lateral to one-third of the axillary artery, while the medial cord was found medial to the same one-third of the axillary artery. The posterior cord was located posterior to one-third of the artery.
Subsequently, the anatomical landmarks related to the course of each of the terminal branches were also noted. The musculocutaneous nerve, which is the lateral cord’s terminal branch, originates/emerges at the inferolateral border of the pectoralis minor muscle. The nerve then pierced the coracobrachialis muscle (lower half of the muscle) to travel inferiorly between the biceps brachii and brachioradialis muscles. Proximal to the cubital fossa, the nerve continued into the forearm as the lateral cutaneous nerve. The axillary nerve branched off the posterior cord to travel posteriorly through the quadrangular space to enter into the posterior compartment of the arm. It then travels inferolateral on the subscapularis muscle to further split into anterior and posterior branches. The radial nerve (terminal branch of the posterior cord) travels posteriorly through the triangular interval to enter the arm’s posterior compartment. Once there, the nerve traveled inferiorly in the radial groove towards the lateral epicondyle. It then entered the cubital fossa anterior to the lateral epicondyle to terminate into its superficial sensory and deep motor branches.
The median nerve traveled inferiorly down the arm, anterior to the axillary artery, and lateral to the brachial artery. At the origin of the brachioradialis muscle, the median nerve crossed over the brachial artery to lie medial to the artery while entering the cubital fossa. Then, the nerve traveled through the flexor digitorum profundus and flexor digitorum superficialis muscles in the forearm while giving off two major branches. It then traveled through the carpal tunnel to enter the hand before terminating into two branches. Lastly, the ulnar nerve descended the arm, between the axillary artery and vein. Midway down the artery, the nerve shifted to lie medial to the brachial artery. It then pierced the fascial septum to enter the posterior compartment of the arm to travel posterior to the medial epicondyle to enter the forearm. In the forearm, the nerve traveled deep to the flexor carpi ulnaris towards the wrist joint. At the joint, the nerve was found superficial to the flexor retinaculum of the hand and medial to the ulnar artery while entering the hand.
5. Conclusion
A thorough understanding of all relevant anatomical landmarks is mandatory for any successful procedure. Common techniques such as BP blocks require detailed anatomical literature due to the complexity and variability of the plexus. The mean length of the trunks was 37.3±2.5 mm, and the cords 47±1.8 mm. The mean length of the terminal branches ranged from 65 to 220 mm. Results from this study will add to the understanding of the anatomy of the BP and further assist clinicians in pre- and perioperative surgical planning.
Limitations and recommendation
A major limitation of this study was the sample size. Therefore, we recommend future studies with a larger sample size together with the aid of imagining modalities such as ultrasound guidance to fully evaluate the anatomy of the BP. Additionally, as this was a retrospective investigation using already embalmed cadavers, tissue shrinkage may influence the measurements.
Ethical Considerations
Compliance with ethical guidelines
Ethical approval was obtained from the Sefako Makgatho Health Sciences University, Research Ethics Committee (SMUREC) (Code: SMUREC/M/165/2020:PG).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and study design: Hazel Hlongwan and Govender-Davies; Data acquisition: Hazel Hlongwan and Sashrika Pillay-Addinal; Data analysis and data interpretation: Hazel Hlongwan; Revising the manuscript for critically for important intellectual content: Sashrika Pillay-Addinal and Sabashnee Govender-Davies; Drafting the article, and final approval: Sabashnee Govender-Davies.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank everyone who was involved in conducting this research.
References
- Kirik A, Mut SE, Daneyemez MK, Seçer Hİ. Anatomical variations of brachial plexus in fetal cadavers. Turkish Neurosurgery. 2017. [DOI:10.5137/1019-5149.JTN.21339-17.2] [PMID]
- Park HR, Lee GS, Kim IS, Chang JC. Brachial plexus injury in adults. The Nerve. 2017; 3(1):1-11. [DOI:10.21129/nerve.2017.3.1.1]
- Lee JP, Chang JC, Cho SJ, Park HK, Choi SK, Bae HG. A morphometric aspect of the brachial plexus in the periclavicular region. Journal of Korean Neurosurgical Society. 2009; 46(2):130-5. [DOI:10.3340/jkns.2009.46.2.130] [PMID]
- Millesi H. Surgical management of brachial plexus injuries. The Journal of Hand Surgery. 1977; 2(5):367-78. [DOI:10.1016/S0363-5023(77)80046-4] [PMID]
- Jamuna M. Clinically significant variations of the cords of the brachial plexus in relation to axillary artery. International Journal of Anatomical Variations. 2011; 4(1):9-11. [Link]
- Emamhadi M, Chabok SY, Samini F, Alijani B, Behzadnia H, Firozabadi FA, et al. Anatomical variations of brachial plexus in adult cadavers; A descriptive study. Archives of Bone and Joint Surgery. 2016; 4(3):253-8. [PMID]
- Bonnel F, Rabischong P. Anatomie et systématisation du plexus brachial de l’adulte, Anatomia Clinica. 1980; 2(3):289-100. [Link]
- Zhong LY, Wang AP, Hong L, Chen SH, Wang XQ, Lv YC, et al. Microanatomy of the brachial plexus roots and its clinical significance. Surgical and Radiologic Anatomy. 2017; 39(6):601-10. [DOI:10.1007/s00276-016-1784-9] [PMID]
- Neto JHS, Neto BC, Eiras ABD, Botelho RHS, Carmo JMM, Passos MARF. The 2-dimensional and 3-dimensional anatomy of the adult brachial plexus divisions and cords. Hand (N Y). 2022; 17(1):50-4. [DOI:10.1177/1558944720906510] [PMID]
- Kerr AT. The brachial plexus of nerves in man, the variations in its formation and branches. American Journal of Anatomy. 1918; 23(2):285-395. [DOI:10.1002/aja.1000230205]
- Cunningham DJ. The value of nerve-supply in the determination of muscular homologies and anomalies. Journal of Anatomy and Physiology. 1890; 25(1):31-40. [PMID]
- Chaudhary P, Singla R, Kalsey G, Arora K. A four trunked brachial plexus and a post fixed brachial plexus: A conjunction or a co-incidence? Report of three cases. Clinical Anatomy (New York, N.Y.). 2012; 25(5):593-600. [DOI:10.1002/ca.21287] [PMID]
Type of Study: Original |
Subject:
Gross Anatomy
Received: 2022/03/7 | Accepted: 2022/08/3 | Published: 2022/07/1
Received: 2022/03/7 | Accepted: 2022/08/3 | Published: 2022/07/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
