Wed, Jul 9, 2025
Volume 15, Issue 1 (Winter & Spring 2018)
ASJ 2018, 15(1): 37-40 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Voshtani S H, Salari A, Nasiri E, Heidarnejad Z, Voshtani S M. Integrated Percutaneous Atrial Septal Defect Occlusion and Pulmonary Balloon Valvuloplasty. ASJ 2018; 15 (1) :37-40
URL: http://anatomyjournal.ir/article-1-152-en.html
URL: http://anatomyjournal.ir/article-1-152-en.html
Seyed Hassan Voshtani1 
 , Arsalan Salari1 , Ebrahim Nasiri1 , Zohre Heidarnejad1 , Seyed Mahsa Voshtani1
, Arsalan Salari1 , Ebrahim Nasiri1 , Zohre Heidarnejad1 , Seyed Mahsa Voshtani1
, Arsalan Salari1 , Ebrahim Nasiri1 , Zohre Heidarnejad1 , Seyed Mahsa Voshtani1
1- Guilan Interventional Cardiovascular Research Center, Heshmat Hospital, Guilan University of Medical Sciences, Rasht, Iran.
Full-Text [PDF 486 kb]
(1383 Downloads)
| Abstract (HTML) (4621 Views)
.jpg)

Full-Text: (2070 Views)
1. Introduction
Atrial Septal Defect (ASD) is one the most common congenital heart diseases during childhood. They contribute to 7%-10% of all cardiac anomalies. Today, ASD closure is done by occlutech device via cardiac catheterization. ASD repair with transcatheter technique has shown high closure rate. The benefit of the percutaneous approach has been well demonstrated in the pediatric population. Coexistence of severe Pulmonary Stenosis (PS) and a large defect in atrial septum is rare. When these two problems coexist, the result is inhibition of remarkable left-to-right shunt by obstruction of the Right Ventricle (RV) output flow, which will preserve the pulmonary bed up to adulthood. In this paper, we explain an effective and feasible combined percutaneous approach for treating these two problems.
Transcatheter pulmonary valvuloplasty is the treatment of choice in isolated pulmonary valve stenosis; transcatheter closure of secundum atrial septal defect with occlutech device is an efficient and safe method, with great success rate in the long-term [1, 2]. There are few case reports of treating valvular PS and secundum ASD together by transcatheter strategy.
2. Case Presentation
A 5-year-old girl was referred by pediatric cardiologist for the treatment of her severe valvular PS and large ASD. She had a history of exertional dyspnea and palpitation.
Electrocardiogram showed right axis deviation, hypertrophy of right ventricle and right atrium as well as right bundle-branch block. Chest x-ray revealed moderate cardiomegaly, bulged main pulmonary artery, and increased marking of pulmonary vasculature. The echocardiography showed a large secundum ASD with a size of 16 mm with appropriate rims and severe pulmonary valvular stenosis with a peak systolic pressure gradient of 62 mm Hg and also poststenotic dilation in the main pulmonary artery. The patient was picked up for closure of ASD by transcatheter procedure and balloon pulmonary valvuloplasty [1, 2].
In cardiac catheterization, the right ventricular pressure was 78 mm Hg and pressure gradient across the pulmonary valve was 62 mm Hg, also the ratio of pulmonary blood flow to systemic blood flow (QP/QS) was 2.7/1 (left to right shunt). Anteroposterior and lateral views in the angiography of right ventricle showed severe valvular PS and poststenotic dilation. Left Anterior Oblique (LAO) view in left ventricular angiogram showed normal ventriculography. Right upper Pulmonary Vein (PV) injection in hepatoclavicular projection revealed a large size ASD with good margins. Diameter of the ASD size by balloon was 16 mm (Figure 1 shows the assessment of the stretched diameter of the atrial septal defect with a sizing balloon catheter).
Pulmonary valve annulus diameter was 15-16 mm. All procedure was implemented under light general anesthesia and transthoracic fluoroscopy guide. Pulmonary valvuloplasty was performed with an 18/30 Tyshak balloon. The valvuloplasty was performed by 6 inflation with 2
Atrial Septal Defect (ASD) is one the most common congenital heart diseases during childhood. They contribute to 7%-10% of all cardiac anomalies. Today, ASD closure is done by occlutech device via cardiac catheterization. ASD repair with transcatheter technique has shown high closure rate. The benefit of the percutaneous approach has been well demonstrated in the pediatric population. Coexistence of severe Pulmonary Stenosis (PS) and a large defect in atrial septum is rare. When these two problems coexist, the result is inhibition of remarkable left-to-right shunt by obstruction of the Right Ventricle (RV) output flow, which will preserve the pulmonary bed up to adulthood. In this paper, we explain an effective and feasible combined percutaneous approach for treating these two problems.
Transcatheter pulmonary valvuloplasty is the treatment of choice in isolated pulmonary valve stenosis; transcatheter closure of secundum atrial septal defect with occlutech device is an efficient and safe method, with great success rate in the long-term [1, 2]. There are few case reports of treating valvular PS and secundum ASD together by transcatheter strategy.
2. Case Presentation
A 5-year-old girl was referred by pediatric cardiologist for the treatment of her severe valvular PS and large ASD. She had a history of exertional dyspnea and palpitation.
Electrocardiogram showed right axis deviation, hypertrophy of right ventricle and right atrium as well as right bundle-branch block. Chest x-ray revealed moderate cardiomegaly, bulged main pulmonary artery, and increased marking of pulmonary vasculature. The echocardiography showed a large secundum ASD with a size of 16 mm with appropriate rims and severe pulmonary valvular stenosis with a peak systolic pressure gradient of 62 mm Hg and also poststenotic dilation in the main pulmonary artery. The patient was picked up for closure of ASD by transcatheter procedure and balloon pulmonary valvuloplasty [1, 2].
In cardiac catheterization, the right ventricular pressure was 78 mm Hg and pressure gradient across the pulmonary valve was 62 mm Hg, also the ratio of pulmonary blood flow to systemic blood flow (QP/QS) was 2.7/1 (left to right shunt). Anteroposterior and lateral views in the angiography of right ventricle showed severe valvular PS and poststenotic dilation. Left Anterior Oblique (LAO) view in left ventricular angiogram showed normal ventriculography. Right upper Pulmonary Vein (PV) injection in hepatoclavicular projection revealed a large size ASD with good margins. Diameter of the ASD size by balloon was 16 mm (Figure 1 shows the assessment of the stretched diameter of the atrial septal defect with a sizing balloon catheter).
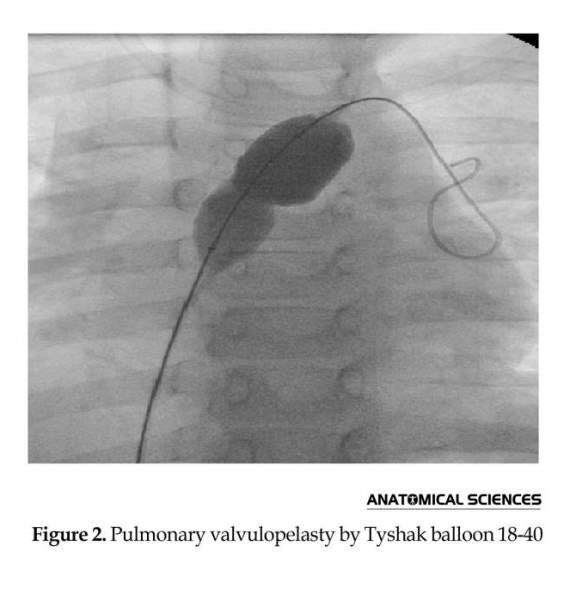
Pulmonary valve annulus diameter was 15-16 mm. All procedure was implemented under light general anesthesia and transthoracic fluoroscopy guide. Pulmonary valvuloplasty was performed with an 18/30 Tyshak balloon. The valvuloplasty was performed by 6 inflation with 2
atmosphere pressure (Figure 2). PG pressure reduced to 18 mm Hg without any complication. The sizing of balloon showed a 16 mm ASD diameter that was closed by using an 18 mm occlutech septal occluder (Figure 3). There was no remaining shunt and complication on transthoracic echocardiography performed immediately and 2 hours after implantation of device. On follow up, there was no residual shunt or notable gradient pressure over the pulmonary valve after 1, 3, 6, 9, and 12 months.
3. Discussion
Improvements in interventional cardiology have offered new therapeutic options for patients suffering from congenital heart diseases. In this regard, pulmonary balloon valvuloplasty with isolated valvular PS has become a treatment of choice. In selected patients, closure of secundum atrial septal defect by transcatheter approach can substitute surgical repair. Effective and trusty interventions via catheter are currently available in many countries for closure of ASD, Ventricular Septal Defect (VSD), and Patent Ductus Arteriosus (PDA).
However, transcatheter treatment of valvular PS and large ASD at the same time is uncommon. Yib et al. presented the first case of simultaneous treatment of balloon pulmonary valvuloplasty and atrial septal defect in 1997 in a 7-year-old girl. In recent times, there was an increase in the number of reports on concurrent transcatheter therapy of valvular PS and secundum ASD [1-4]. Numerous factors including size of ASD, adequate ASD rim, and degree of pressure gradient across the pulmonary valve affects the decision to merge pulmonary valve dilation and device closure of ASD.
In our patient, we first performed pulmonary valvuloplasty to minimize catheter manipulation after implantation of ASD device. Our patient’s symptoms and signs got better after combined therapy of critical PS and ASD. The main benefits of percutaneous closure of ASD are short hospital stage, absence of thoracotomy, open heart surgery or admission to an intensive care unit, and also avoiding further surgical scar and postoperative pain.
However complete occlusion of the ASD and immediate relief of pulmonary obstruction was achieved at the end of the procedure and confirmed by transthoracic echocardiography the next day, 1, 6, and 12 months and yearly there after [5-9]. In conclusion, the combined transcatheter closure of ASD and pulmonary balloon valvuloplasty is feasible, effective, and achieves a delighting outcome.
Acknowledgements
We acknowledge the director and staff of Cardiovascular Diseases Research Center of Guilan University of Medical Sciences. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of Interest
The authors declared no conflict of interests.
References
3. Discussion
Improvements in interventional cardiology have offered new therapeutic options for patients suffering from congenital heart diseases. In this regard, pulmonary balloon valvuloplasty with isolated valvular PS has become a treatment of choice. In selected patients, closure of secundum atrial septal defect by transcatheter approach can substitute surgical repair. Effective and trusty interventions via catheter are currently available in many countries for closure of ASD, Ventricular Septal Defect (VSD), and Patent Ductus Arteriosus (PDA).
However, transcatheter treatment of valvular PS and large ASD at the same time is uncommon. Yib et al. presented the first case of simultaneous treatment of balloon pulmonary valvuloplasty and atrial septal defect in 1997 in a 7-year-old girl. In recent times, there was an increase in the number of reports on concurrent transcatheter therapy of valvular PS and secundum ASD [1-4]. Numerous factors including size of ASD, adequate ASD rim, and degree of pressure gradient across the pulmonary valve affects the decision to merge pulmonary valve dilation and device closure of ASD.
In our patient, we first performed pulmonary valvuloplasty to minimize catheter manipulation after implantation of ASD device. Our patient’s symptoms and signs got better after combined therapy of critical PS and ASD. The main benefits of percutaneous closure of ASD are short hospital stage, absence of thoracotomy, open heart surgery or admission to an intensive care unit, and also avoiding further surgical scar and postoperative pain.
However complete occlusion of the ASD and immediate relief of pulmonary obstruction was achieved at the end of the procedure and confirmed by transthoracic echocardiography the next day, 1, 6, and 12 months and yearly there after [5-9]. In conclusion, the combined transcatheter closure of ASD and pulmonary balloon valvuloplasty is feasible, effective, and achieves a delighting outcome.
Acknowledgements
We acknowledge the director and staff of Cardiovascular Diseases Research Center of Guilan University of Medical Sciences. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of Interest
The authors declared no conflict of interests.
References
- Tomasov P, Linhartova K, Antonova P, Adlova R, Alan D, Veselka J. Combined percutaneous treatment of atrial septal defect and pulmonic or aortic stenosis in adult patients. Archives of Medical Science. 2010; 6:976–80. doi: 10.5114/aoms.2010.19312
- Yip W, Chan K, Godman M. Simultaneous Transcatheter Valvuloplasty and Amplatzer Septal Occlusion for Pulmonary Valvar Stenosis and Secundum Atrial Septa. Defect. 1998; 27(4):578-81. PMID: 9791671
- King TD, Mills NL. Historical perspectives on ASD device closure. Transcatheter Closure of ASDs and PFOs, A Comprehensive Assessment. Minneapolis, Minnesota: Cardiotext Publishing; 2010.
- Mashman WE, King SB, Jacobs WC, Ballard WL. Two cases of late embolization of Amplatzer septal occluder devices to the pulmonary artery following closure of secundum atrial septal defects. Catheterization and Cardiovascular Interventions. 2005; 65(4):588–92. doi: 10.1002/ccd.20429
- Moss AJ, Allen HD. Moss and Adams’ heart disease in infants, children, and adolescents: including the fetus and young adult. Philadelphia: Lippincott Williams & Wilkins; 2008.
- Costache V, Chavanon O, Thony F, Blin D. Aortic arch embolization of an Amplatzer occluder after an atrial septal defect closure: hybrid operative approach without circulatory arrest. European Journal of Cardio-Thoracic Surgery. 2005; 28(2):340–2. doi: 10.1016/j.ejcts.2005.04.022
- Knirsch W, Dodge-Khatami A, Balmer C, Peuster M, Kadner A, Weiss M, et al. Aortic sinus-left atrial fistula after interventional closure of atrial septal defect. Catheterization and Cardiovascular Interventions. 2005; 66(1):10–3. doi: 10.1002/ccd.20436
- Varma C, Benson LN, Silversides C, Yip J, Warr MR, Webb G, et al. Outcomes and alternative techniques for device closure of the large secundum atrial septal defect. Catheterization and Cardiovascular Interventions. 2003; 61(1):131–9. doi: 10.1002/ccd.10700
- Thanopoulos B (Vasilios) D, Laskari CV, Tsaousis GS, Zarayelyan A, Vekiou A, Papadopoulos GS. Closure of Atrial Septal Defects With the Amplatzer Occlusion Device: Preliminary Results. Journal of the American College of Cardiology. 1998; 31(5):1110–6. doi: 10.1016/s0735-1097(98)00039-4
Type of Study: Original |
Subject:
Gross Anatomy
Received: 2016/09/19 | Accepted: 2017/12/25 | Published: 2018/01/1
Received: 2016/09/19 | Accepted: 2017/12/25 | Published: 2018/01/1
References
1. Tomasov P, Linhartova K, Antonova P, Adlova R, Alan D, Veselka J. Combined percutaneous treatment of atrial septal defect and pulmonic or aortic stenosis in adult patients. Archives of Medical Science. 2010; 6:976–80. doi: 10.5114/aoms.2010.19312 [DOI:10.5114/aoms.2010.19312]
2. Yip W, Chan K, Godman M. Simultaneous Transcatheter Valvuloplasty and Amplatzer Septal Occlusion for Pulmonary Valvar Stenosis and Secundum Atrial Septa. Defect. 1998; 27(4):578-81. PMID: 9791671
3. King TD, Mills NL. Historical perspectives on ASD device closure. Transcatheter Closure of ASDs and PFOs, A Comprehensive Assessment. Minneapolis, Minnesota: Cardiotext Publishing; 2010.
4. Mashman WE, King SB, Jacobs WC, Ballard WL. Two cases of late embolization of Amplatzer septal occluder devices to the pulmonary artery following closure of secundum atrial septal defects. Catheterization and Cardiovascular Interventions. 2005; 65(4):588–92. doi: 10.1002/ccd.20429 [DOI:10.1002/ccd.20429]
5. Moss AJ, Allen HD. Moss and Adams' heart disease in infants, children, and adolescents: including the fetus and young adult. Philadelphia: Lippincott Williams & Wilkins; 2008.
6. Costache V, Chavanon O, Thony F, Blin D. Aortic arch embolization of an Amplatzer occluder after an atrial septal defect closure: hybrid operative approach without circulatory arrest. European Journal of Cardio-Thoracic Surgery. 2005; 28(2):340–2. doi: 10.1016/j.ejcts.2005.04.022 [DOI:10.1016/j.ejcts.2005.04.022]
7. Knirsch W, Dodge-Khatami A, Balmer C, Peuster M, Kadner A, Weiss M, et al. Aortic sinus-left atrial fistula after interventional closure of atrial septal defect. Catheterization and Cardiovascular Interventions. 2005; 66(1):10–3. doi: 10.1002/ccd.20436 [DOI:10.1002/ccd.20436]
8. Varma C, Benson LN, Silversides C, Yip J, Warr MR, Webb G, et al. Outcomes and alternative techniques for device closure of the large secundum atrial septal defect. Catheterization and Cardiovascular Interventions. 2003; 61(1):131–9. doi: 10.1002/ccd.10700 [DOI:10.1002/ccd.10700]
9. Thanopoulos B (Vasilios) D, Laskari CV, Tsaousis GS, Zarayelyan A, Vekiou A, Papadopoulos GS. Closure of Atrial Septal Defects With the Amplatzer Occlusion Device: Preliminary Results. Journal of the American College of Cardiology. 1998; 31(5):1110–6. doi: 10.1016/s0735-1097(98)00039-4 [DOI:10.1016/S0735-1097(98)00039-4]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
