Wed, May 27, 2026
Volume 20, Issue 2 (Summer & Autumn 2023)
ASJ 2023, 20(2): 39-44 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Eftekhar-Vaghefi S H, Raygan S P, Dehghani-Soltani S, Babaee A. A Cadaveric Study of the Accessory Phrenic Nerve: Assessment of Prevalence, Origin, and Clinical Significance. ASJ 2023; 20 (2) :39-44
URL: http://anatomyjournal.ir/article-1-250-en.html
URL: http://anatomyjournal.ir/article-1-250-en.html
Seyed Hassan Eftekhar-Vaghefi1 

 , Seyed Parviz Raygan1 , Samereh Dehghani-Soltani2 , Abdolreza Babaee2
, Seyed Parviz Raygan1 , Samereh Dehghani-Soltani2 , Abdolreza Babaee2
, Seyed Parviz Raygan1 , Samereh Dehghani-Soltani2 , Abdolreza Babaee2
1- Department of Anatomical Sciences, School of Medicine, Kerman University of Medical Sciences, Kerman, Iran.
2- Department of Anatomical Sciences, School of Medicine, Rafsanjan University of Medical Sciences, Rafsanjan, Iran.
2- Department of Anatomical Sciences, School of Medicine, Rafsanjan University of Medical Sciences, Rafsanjan, Iran.
Full-Text [PDF 2143 kb]
(378 Downloads)
| Abstract (HTML) (2280 Views)
Full-Text: (609 Views)
Introduction
The diaphragm is the primary muscle of inspiration, with the phrenic nerves serving as its sole motor innervation [1]. Many complications following cervical and thoracic surgeries are associated with phrenic nerve damage and its branches. Therefore, an accurate anatomical description of the phrenic nerve and its branches is clinically significant [2].
The accessory phrenic nerve (APN) typically originates from the fifth cervical nerve and connects to the phrenic nerve via the nerve to the subclavius [3, 4]. It runs lateral to the phrenic nerve, descending behind or, in some cases, anterior to the subclavian vein, usually joining the phrenic nerve near the first rib [5, 6]. However, variations have been reported, including junctions near the lung hilum [5, 6]. Previous studies have demonstrated significant variability in the prevalence and origin of APNs [7, 8]. Despite its importance, anatomical textbooks often provide limited information on the APN, and no data on its incidence in the Iranian population exist. Therefore, this study aimed to evaluate the prevalence and anatomical variations of the APN.
Materials and Methods
This study involved the dissection of 26 adult male cadavers (aged 20–65 years), yielding 52 nerve specimens. Dissections were conducted using Grant’s standard method to examine the phrenic nerve branches and the presence, course, and origin of APNs. A stereomicroscope was used to visualize small branches. Dissections were performed at the Afzalipour Faculty of Medical Sciences and the forensic hall in Kerman, Iran. Written consent was obtained from the cadavers’ families prior to the study. Data were recorded in pre-prepared tables and analyzed using SPSS software, version 16.
Results
The total prevalence of APN was 30.77% (8 of 26 cadavers). In five cases, APN was bilateral, while in three cases, it was unilateral (two left-sided and one right-sided) (Table 1).

In five cadavers, the APN originated from the root of the fifth cervical nerve, while in three cases, it branched from the nerve to the subclavius. In four cadavers, the APN joined the phrenic nerve at the thoracic inlet, while in one cadaver, the junction occurred near the lower part of the lung hilum. In the remaining three cases, the junction was located between the thoracic inlet and the upper part of the lung hilum. In all eight cases, the APN traversed posterior to the subclavian vein.
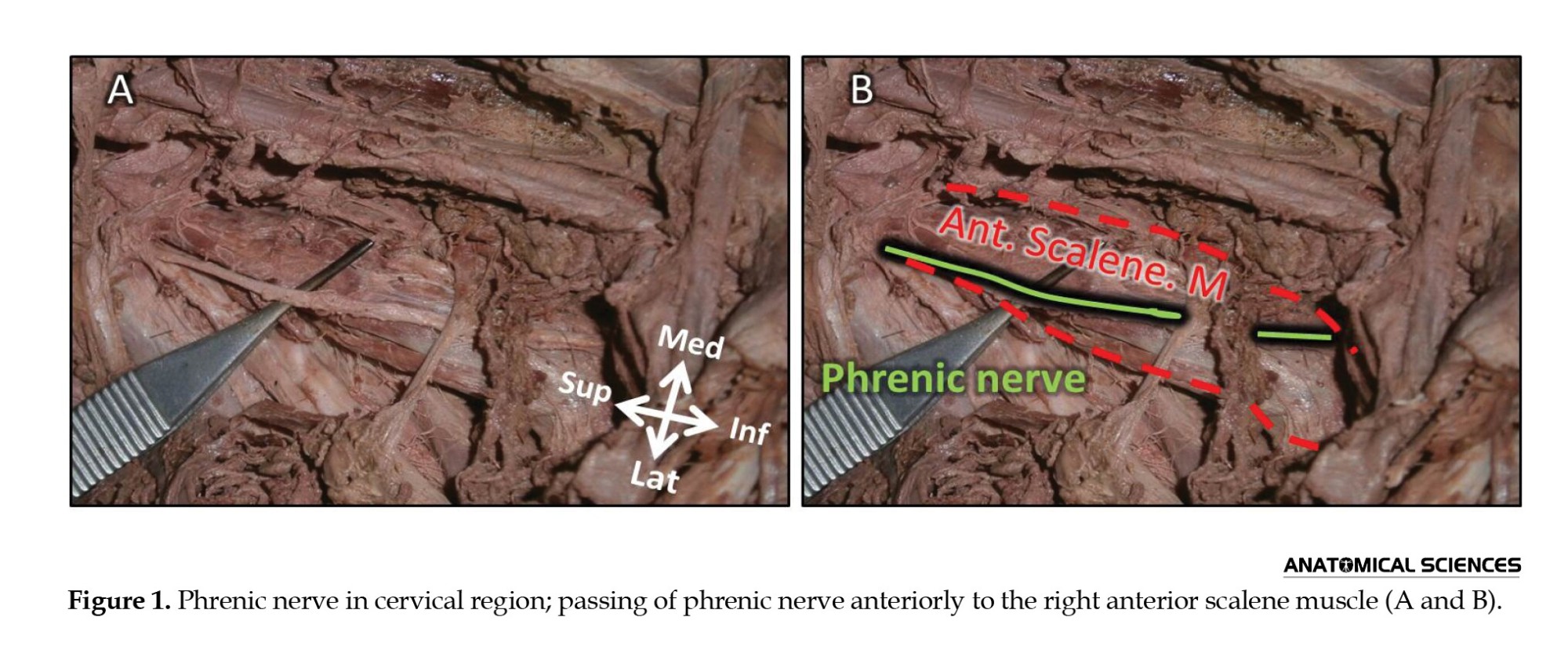
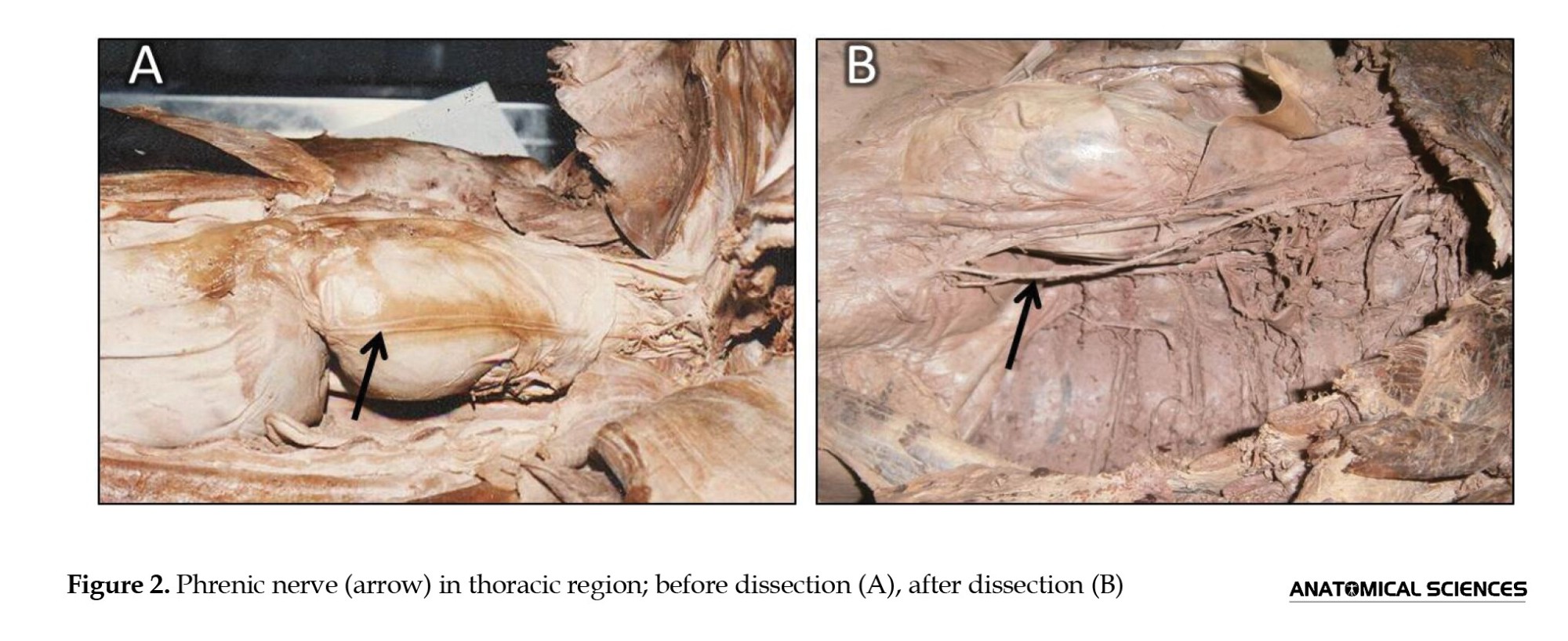
The anatomical variations observed in this study were consistent with previous reports. In all cadavers, the phrenic nerve was formed by the anterior branches of the third, fourth, and fifth cervical nerves. Additionally, the anatomical relationships of the phrenic nerve in the cervical (Figure 1) and thoracic (Figure 2) regions were examined, showing no deviations from prior studies.
Discussion
A thorough understanding of nerve, muscle, and vascular variations is essential in surgery to prevent iatrogenic injuries [9-13]. Phrenic nerve injury in the cervical region can lead to unilateral diaphragmatic paralysis [14]. However, in cases where an APN is present, it may preserve some diaphragmatic function even if the phrenic nerve is compressed or severed [14, 15].
Our study revealed an APN prevalence of 30.77%, lower than the 45% reported by Talbot et al. [16]. The APN commonly originates from the nerve to the subclavius, a pattern observed in three cases in our study. However, in five cadavers, the APN arose from the root of the fifth cervical nerve. Loukas et al. found that this type of APN origin occurred in only 2% of cases [5].
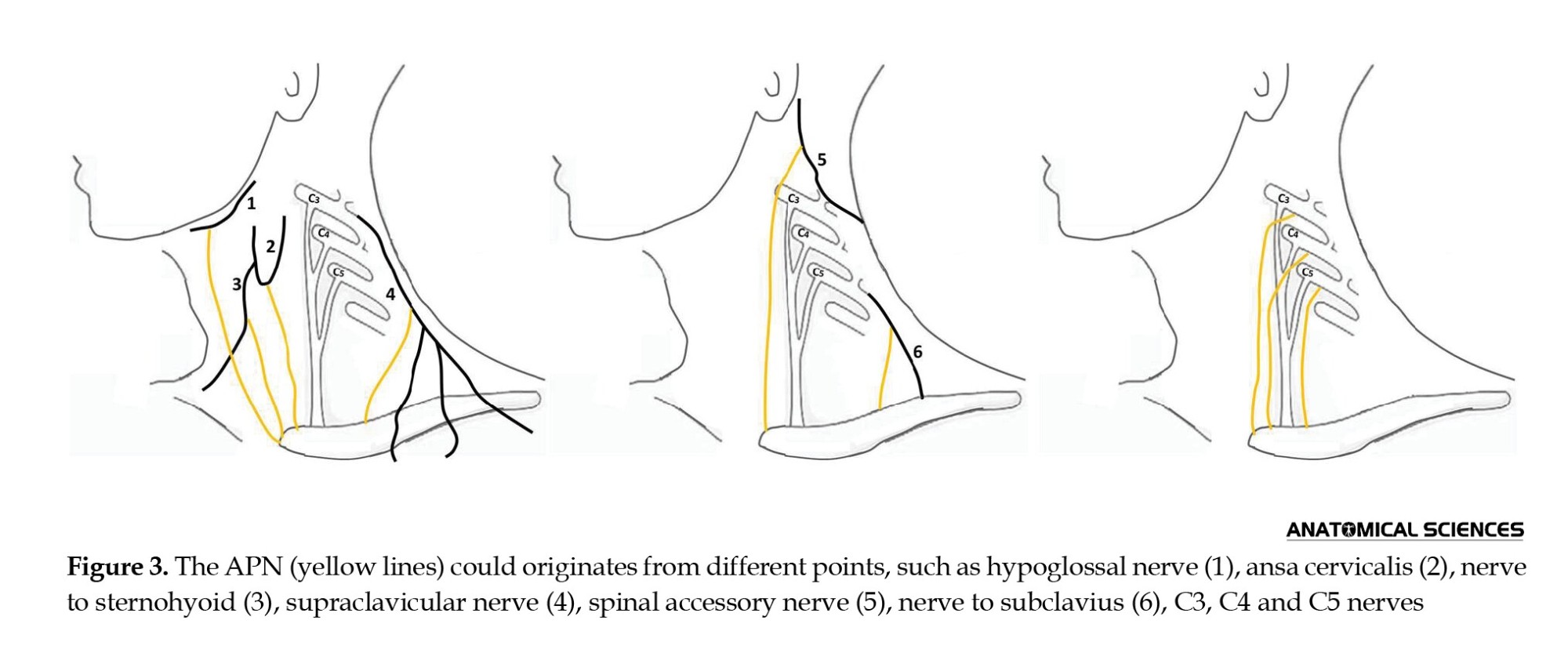
APNs may also arise from spinal nerves C4 or C6, the ansa cervicalis, or the nerve to sternohyoid (Figure 3) [5, 7, 17], but these variations were absent in our study. In some studies, the APN has been reported to traverse through a loop formed by the subclavian vein [8]. Our findings indicated that in all cases, the APN passed posterior to the subclavian vein. Loukas et al. found that in 45.5% of cases, the APN was posterior to the subclavian vein, whereas in 22.2% of cases, it was anterior [5]. Furthermore, they reported that in 9.1% of cases, the APN was medial to the phrenic nerve, while in our study, the APN was lateral to the phrenic nerve in all cases.
Previous studies have reported the absence of C3 and C5 contributions to the phrenic nerve [18-20]. However, in our study, all examined cadavers showed phrenic nerve formation from C3, C4, and C5. Understanding phrenic nerve anatomy and its variations is crucial during cervical and thoracic surgeries to prevent iatrogenic injuries [21-23]. Another clinical implication of APN arises during nerve blocks in the lower cervical region, as transient diaphragmatic paralysis has been reported, possibly due to phrenic nerve or APN involvement [24-26].
One limitation of this study is that it was conducted in a single province. A broader investigation across multiple Iranian provinces is recommended to provide a more comprehensive understanding of APN prevalence in the Iranian population.
Conclusion
Considering racial anatomical differences, collecting anatomical data from diverse populations is essential. Understanding the prevalence, variable origins, and anatomical relationships of the APN can assist clinicians and surgeons in optimizing thoracic surgical procedures.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Rafsanjan University of Medical Sciences, Rafsanjan Iran (Code: IR.RUMS.REC.1402.035).
Funding
This study was financially supported by Rafsanjan University of Medical Sciences.
Authors' contributions
Conceptualization, methodology, funding acquisition: Seyed Hassan Eftekhar-Vaghefi and Abdolreza Babaee; Review and editing: Samereh Dehghani-Soltani; Physical examination: Seyed Parviz Raygan.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgments
The authors appreciate the families of the cadavers and colleagues at the Kerman Forensic Department, Kerman, Iran.
References
The diaphragm is the primary muscle of inspiration, with the phrenic nerves serving as its sole motor innervation [1]. Many complications following cervical and thoracic surgeries are associated with phrenic nerve damage and its branches. Therefore, an accurate anatomical description of the phrenic nerve and its branches is clinically significant [2].
The accessory phrenic nerve (APN) typically originates from the fifth cervical nerve and connects to the phrenic nerve via the nerve to the subclavius [3, 4]. It runs lateral to the phrenic nerve, descending behind or, in some cases, anterior to the subclavian vein, usually joining the phrenic nerve near the first rib [5, 6]. However, variations have been reported, including junctions near the lung hilum [5, 6]. Previous studies have demonstrated significant variability in the prevalence and origin of APNs [7, 8]. Despite its importance, anatomical textbooks often provide limited information on the APN, and no data on its incidence in the Iranian population exist. Therefore, this study aimed to evaluate the prevalence and anatomical variations of the APN.
Materials and Methods
This study involved the dissection of 26 adult male cadavers (aged 20–65 years), yielding 52 nerve specimens. Dissections were conducted using Grant’s standard method to examine the phrenic nerve branches and the presence, course, and origin of APNs. A stereomicroscope was used to visualize small branches. Dissections were performed at the Afzalipour Faculty of Medical Sciences and the forensic hall in Kerman, Iran. Written consent was obtained from the cadavers’ families prior to the study. Data were recorded in pre-prepared tables and analyzed using SPSS software, version 16.
Results
The total prevalence of APN was 30.77% (8 of 26 cadavers). In five cases, APN was bilateral, while in three cases, it was unilateral (two left-sided and one right-sided) (Table 1).
In five cadavers, the APN originated from the root of the fifth cervical nerve, while in three cases, it branched from the nerve to the subclavius. In four cadavers, the APN joined the phrenic nerve at the thoracic inlet, while in one cadaver, the junction occurred near the lower part of the lung hilum. In the remaining three cases, the junction was located between the thoracic inlet and the upper part of the lung hilum. In all eight cases, the APN traversed posterior to the subclavian vein.
The anatomical variations observed in this study were consistent with previous reports. In all cadavers, the phrenic nerve was formed by the anterior branches of the third, fourth, and fifth cervical nerves. Additionally, the anatomical relationships of the phrenic nerve in the cervical (Figure 1) and thoracic (Figure 2) regions were examined, showing no deviations from prior studies.
Discussion
A thorough understanding of nerve, muscle, and vascular variations is essential in surgery to prevent iatrogenic injuries [9-13]. Phrenic nerve injury in the cervical region can lead to unilateral diaphragmatic paralysis [14]. However, in cases where an APN is present, it may preserve some diaphragmatic function even if the phrenic nerve is compressed or severed [14, 15].
Our study revealed an APN prevalence of 30.77%, lower than the 45% reported by Talbot et al. [16]. The APN commonly originates from the nerve to the subclavius, a pattern observed in three cases in our study. However, in five cadavers, the APN arose from the root of the fifth cervical nerve. Loukas et al. found that this type of APN origin occurred in only 2% of cases [5].
APNs may also arise from spinal nerves C4 or C6, the ansa cervicalis, or the nerve to sternohyoid (Figure 3) [5, 7, 17], but these variations were absent in our study. In some studies, the APN has been reported to traverse through a loop formed by the subclavian vein [8]. Our findings indicated that in all cases, the APN passed posterior to the subclavian vein. Loukas et al. found that in 45.5% of cases, the APN was posterior to the subclavian vein, whereas in 22.2% of cases, it was anterior [5]. Furthermore, they reported that in 9.1% of cases, the APN was medial to the phrenic nerve, while in our study, the APN was lateral to the phrenic nerve in all cases.
Previous studies have reported the absence of C3 and C5 contributions to the phrenic nerve [18-20]. However, in our study, all examined cadavers showed phrenic nerve formation from C3, C4, and C5. Understanding phrenic nerve anatomy and its variations is crucial during cervical and thoracic surgeries to prevent iatrogenic injuries [21-23]. Another clinical implication of APN arises during nerve blocks in the lower cervical region, as transient diaphragmatic paralysis has been reported, possibly due to phrenic nerve or APN involvement [24-26].
One limitation of this study is that it was conducted in a single province. A broader investigation across multiple Iranian provinces is recommended to provide a more comprehensive understanding of APN prevalence in the Iranian population.
Conclusion
Considering racial anatomical differences, collecting anatomical data from diverse populations is essential. Understanding the prevalence, variable origins, and anatomical relationships of the APN can assist clinicians and surgeons in optimizing thoracic surgical procedures.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Rafsanjan University of Medical Sciences, Rafsanjan Iran (Code: IR.RUMS.REC.1402.035).
Funding
This study was financially supported by Rafsanjan University of Medical Sciences.
Authors' contributions
Conceptualization, methodology, funding acquisition: Seyed Hassan Eftekhar-Vaghefi and Abdolreza Babaee; Review and editing: Samereh Dehghani-Soltani; Physical examination: Seyed Parviz Raygan.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgments
The authors appreciate the families of the cadavers and colleagues at the Kerman Forensic Department, Kerman, Iran.
References
- Snell RS. Clinical anatomy by regions. Philadelphia: Lippincott Williams & Wilkins; 2012. [Link]
- Deng Y, Byth K, Paterson HS. Phrenic nerve injury associated with high free right internal mammary artery harvesting. The Annals of Thoracic Surgery. 2003; 76(2):459-63. [DOI:10.1016/S0003-4975(03)00511-3] [PMID]
- Prakash PL, Prabhu L, Madhyastha S, Singh G. A variation of the phrenic nerve: Case report and review. Singapore Medical Journal. 2007; 48(12):1156-7. [PMID]
- Dayal S, Ky M. The variations in the roots of origin of the phrenic nerve. Journal of Mahatma Gandhi Institute of Medical Sciences. 2009; 14:24-7. [Link]
- Loukas M, Kinsella CR, Louis RG, Gandhi S, Curry B. Surgical anatomy of the accessory phrenic nerve. The Annals of Thoracic Surgery. 2006; 82(5):1870-5. [DOI:10.1016/j.athoracsur.2006.05.098] [PMID]
- Moore KL, Dalley AF, Agur AM. Clinically Oriented Anatomy. Philadelphia: Lippincott Williams & Wilkins; 2018. [Link]
- Graves MJ, Henry BM, Hsieh WC, Sanna B, PĘkala PA, Iwanaga J, et al. Origin and prevalence of the accessory phrenic nerve: A meta-analysis and clinical appraisal. Clinical Anatomy. 2017; 30(8):1077-82. [Link]
- Codesido M, Guerri Guttenberg R. Right accessory phrenic nerve passing through an annulus of the subclavian vein. Clinical Anatomy. 2008; 21(8):779-80. [DOI:10.1002/ca.20657] [PMID]
- Babaee A, Dehghani Soltani S, Ansari Mohajer J, Eftekhar Vaghefi SH, Ezzatabadipour M. The prevalence of palmaris longus absence in the city of Kerman in Iran and the relevance of age, gender and body side. International Journal of Current Research and Review. 2015; 7(14):45. [Link]
- Dehghani Soltani S, Eftekhar Vaghefi SH, Babaee A. An uncommon variation of the superior laryngeal artery. Anatomical Sciences Journal. 2016; 13(1):63-6. [Link]
- Eftekhar Vaghefi SH, Dehghani Soltani S, Babaee A. Case report: An uncommon anatomical variation of the sciatic nerve. Anatomical Sciences Journal. 2016; 13(4):239-42. [Link]
- Babaee A, Soltani SD, Hasan S, Jahanbani SS, Ezzatabadipour M. Abnormal origin of superior laryngeal artery and its clinical significance. Journal of Kerman University of Medical Sciences. 2017; 24(3):246-9. [Link]
- Rayegan S, Kouhestani H, Babaee A, Shekarreez P, Asafe A, Dehghani Soltani S, et al. [A survey on different types of ear lobule in a Kerman population in 2015 (Persian)]. Journal of Rafsanjan University of Medical Sciences. 2017; 16(2):107-16. [Link]
- Sánchez-Quintana D, Cabrera JA, Climent V, Farré J, Weiglein A, Ho SY. How close are the phrenic nerves to cardiac structures? Implications for cardiac interventionalists. Journal of Cardiovascular Electrophysiology. 2005; 16(3):309-13. [DOI:10.1046/j.1540-8167.2005.40759.x] [PMID]
- Buch E, Vaseghi M, Cesario DA, Shivkumar K. A novel method to prevent phrenic nerve injury during catheter ablation. Heart Rhythm. 2007; 4(1):95. [DOI:10.1016/j.hrthm.2006.09.019] [PMID]
- Talbot R. Anatomical pitfall of subclavian venepuncture. Annals of the Royal College of Surgeons of England. 1978; 60(4):317. [PMID]
- Abdelmotalab MA, Ali QM. Accessory phrenic nerve: case report and literature review. Indian Journal of Basic & Applied Medical Research. 2022; 11(2):62-5. [Link]
- Bigeleisen P. Anatomical variations of the phrenic nerve and its clinical implication for supraclavicular block. British Journal of Anaesthesia. 2003; 91(6):916-7. [DOI:10.1093/bja/aeg254] [PMID]
- Canella C, Demondion X, Delebarre A, Moraux A, Cotten H, Cotten A. Anatomical study of phrenic nerve using ultrasound. European Radiology. 2010; 20(3):659-65. [DOI:10.1007/s00330-009-1579-z] [PMID]
- Hamada T, Usami A, Kishi A, Kon H, Takada S. Anatomical study of phrenic nerve course in relation to neck dissection. Surgical and Radiologic Anatomy. 2015; 37(3):255-8. [DOI:10.1007/s00276-014-1343-1] [PMID]
- Prates Junior A, Vasques L, Bordoni L. Anatomical variations of the phrenic nerve: An actualized review. Journal of Morphology. 2015; 32(1):53-6. [DOI:10.4322/jms.070114]
- Abdunnur SV, Kim DH. Phrenic nerve stimulation: Technology and clinical applications. 2015; 29:64-75. [DOI:10.1159/000434657] [PMID]
- Loukas M, Du Plessis M, Louis RG, Tubbs RS, Wartmann CT, Apaydin N. The subdiaphragmatic part of the phrenic nerve - morphometry and connections to autonomic ganglia. Clinical Anatomy. 2016; 29(1):120-8. [DOI:10.1002/ca.22652] [PMID]
- Lee JH, Cho SH, Kim SH, Chae WS, Jin HC, Lee JS, et al. Ropivacaine for ultrasound guided interscalene block: 5 mL provides similar analgesia but less phrenic nerve paralysis than 10 mL. Canadian Journal of Anesthesia. 2011; 58(11):1001-6. [DOI:10.1007/s12630-011-9568-5] [PMID]
- Van de Perck F, Soetens F, Lebrun C, Lataster A, Verhamme A, Van Zundert J. Phrenic nerve injury after radiofrequency denervation of the cervical medial branches. Pain Practice. 2015; 16(2):E42-5. [DOI:10.1111/papr.12398] [PMID]
- Stundner O, Meissnitzer M, Brummett C, Moser S, Forstner R, Koköfer A, et al. Comparison of tissue distribution, phrenic nerve involvement, and epidural spread in standard vs low volume ultrasound guided interscalene plexus block using contrast magnetic resonance imaging: A randomized, controlled trial. British Journal of Anaesthesia. 2016; 116(3):405-12. [DOI:10.1093/bja/aev550] [PMID]
Type of Study: Original |
Subject:
Gross Anatomy
Received: 2019/07/11 | Accepted: 2025/02/16 | Published: 2023/08/30
Received: 2019/07/11 | Accepted: 2025/02/16 | Published: 2023/08/30
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
