Sun, Jul 26, 2026
Volume 20, Issue 2 (Summer & Autumn 2023)
ASJ 2023, 20(2): 55-62 |
Back to browse issues page



![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Moghadami S, Bahadoran H, Eftekhari Moghadam A, Asadi M H. A New Dissection Method of Lower Limbs for Whole Body Plastination. ASJ 2023; 20 (2) :55-62
URL: http://anatomyjournal.ir/article-1-633-en.html
URL: http://anatomyjournal.ir/article-1-633-en.html



1- Department of Anatomy, School of Medicine, Baqiyatallah University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 526 kb]
(603 Downloads)
| Abstract (HTML) (2493 Views)
Full-Text: (1378 Views)
Introduction
Plastination, pioneered by Gunther von Hagens in 1977, is a technique that preserves biological tissues while maintaining anatomical accuracy [1]. This method has revolutionized medical education by offering long-lasting odorless specimens that resemble living tissues [2]. However, one limitation of plastination is that, after final curing, the resulting specimen becomes rigid and non-flexible, with a plastic-like consistency [3].
Understanding the anatomical structure and function of the lower limbs, including muscles, nerves, and vessels, is crucial for medical students [4]. In this study, we aim to propose a novel dissection approach for lower limb plastination, optimizing tissue preservation and educational value while maintaining anatomical integrity. We dissect the left and right limbs differently. The left limb is dissected, preserving its superficial muscles for standard anatomical study [5], while the superficial muscles of the right limb are removed, exposing deep anatomical structures such as vessels, nerves, and deep muscles. This approach allows for a comparative study of both surface and deep layers in a single specimen.
Materials and Methods
Dissection protocol
The proposed dissection protocol is different from the traditional proximal-to-distal approach. The cadaver was embalmed with a strong fixative and kept moist to prevent desiccation [6]. To optimize plastination, we performed dissection in a distal-to-proximal direction, preserving anatomical structures while minimizing tissue damage [7]. The skin was removed gradually, ensuring that the subcutaneous fat (which can delay plastination) was carefully excised. We dissected the superficial muscles, vessels, and nerves in one limb, while they were removed in the other limb to expose the deep structures. This technique allows for a comprehensive analysis of anatomical layers.
Skin removal
The first step in the dissection process was the skin excision. Directly beneath the skin, there are different layers of subcutaneous tissue, known as superficial fascia. This layer contains cutaneous nerves, adipose tissue, and superficial vascular structures [8]. We had to remove the skin with subcutaneous fat.
The skin was removed using toothed forceps and the scalpel blade [1]. The scalpel blade should be directed deep into the skin to cut the collagen fibers. Cutaneous nerves and superficial veins were dissected and the fat was eliminated to better see the deep fascia. For this purpose, in one lower limb, we dissected the superficial muscles with nerves and vessels, while removing them in the other limb to determine the deep muscles, vessels, and nerves.
Dorsum of the foot and anterior and lateral compartments of the left leg
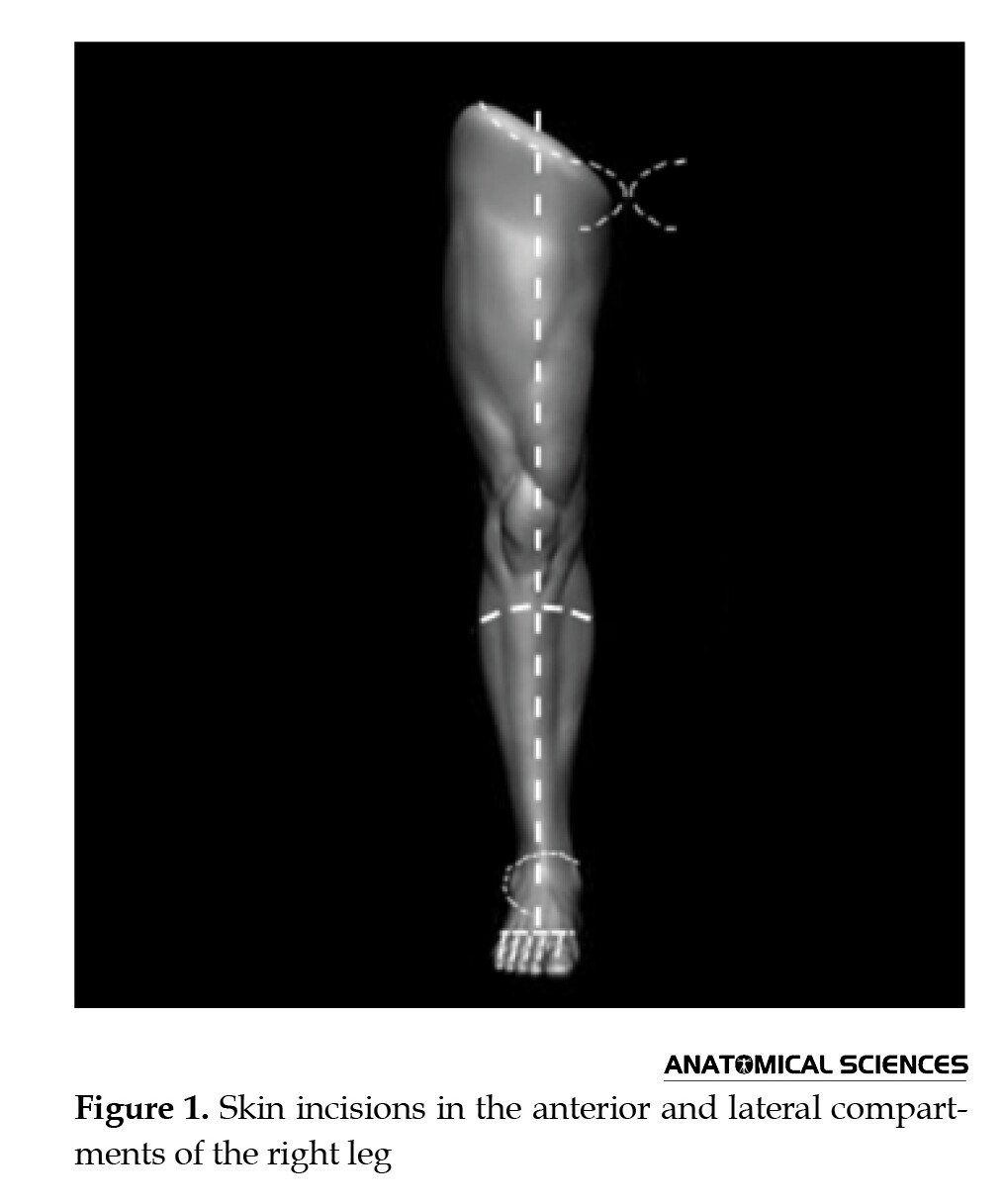
The dorsum of the foot, behind the toes, was incised, followed by more cuts along the dorsal midline of each toe to the proximal end of the nail [9]. Finally, skin was picked up from the dorsum of the foot in the lateral and medial directions. The anterior compartment, consisting of extensor hallucis longus, tibialis anterior, fibularis tertius, and extensor digitorum longus, was dissected. The deep fibular nerve and anterior tibial artery were traced distally. The anatomical path of the dorsalis pedis artery was determined by following it onto the foot [10]. The superior extensor retinaculum is the level at which the anterior tibial artery is located. A distal direction of the anterior tibial artery was then seen. The probe was used to clean the artery. Along this path, it was observed that the anterior tibial artery joins the deep fibular nerve just below the knee. The deep fibular nerve was followed proximally and confirmed to be a branch of the common fibular nerve (Figure 1).
On the foot’s dorsum, the extensor hallucis brevis and extensor digitorum brevis muscles are located beneath the tendons of the extensor digitorum longus muscle. The dorsalis pedis artery is also seen on the dorsum [11]. It runs along the lateral side of the extensor hallucis longus tendon near the ankle in the distal part of the leg. On the leg’s anterior compartment, the superficial fascia remnants were removed [12]. In order to make the crural fascia visible, we identified the anterior surface of the ankle’s superior and inferior extensor retinacula. The tibialis anterior and extensor digitorum longus muscles were separated by fingers. Between the two muscles, the anterior tibial artery was traced proximally.
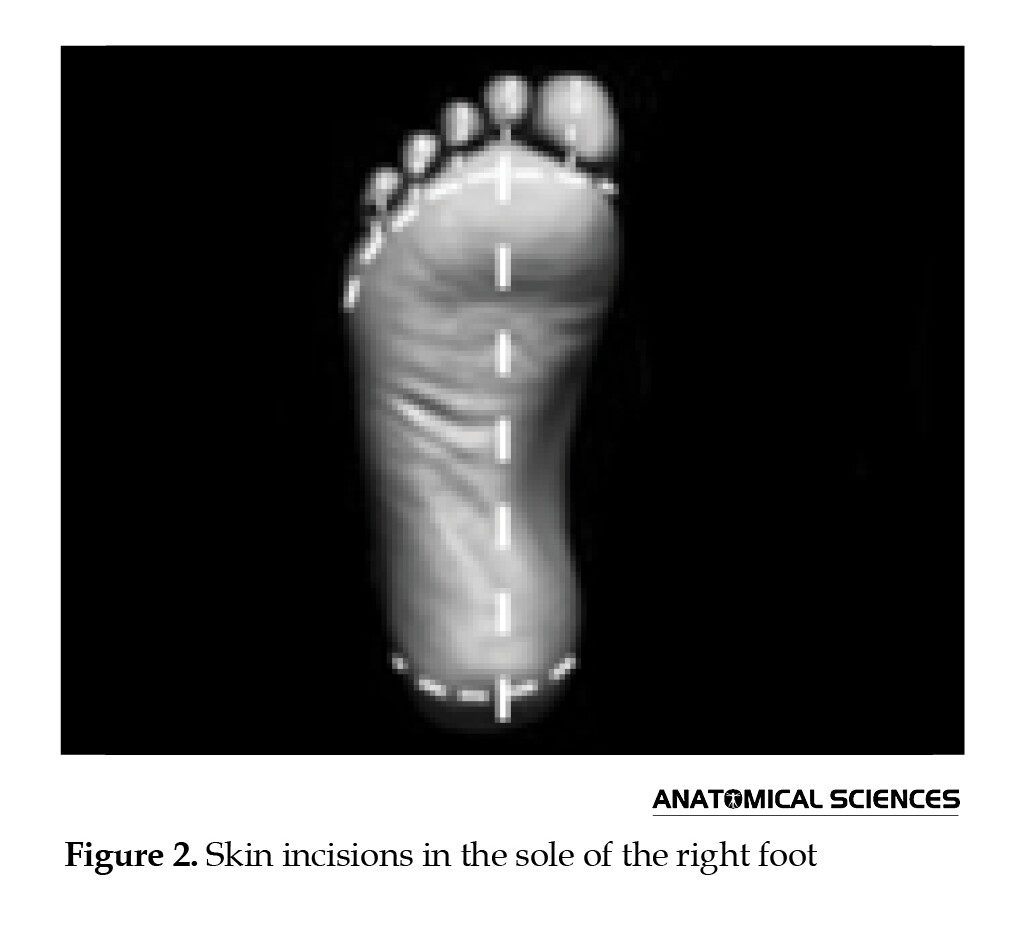
The plantar region of the left foot was also dissected (Figure 2). The foot has a longitudinal arch. The calcaneus (located posteriorly) and the heads of the five metatarsals (located anteriorly) are among the weight-bearing points in the foot [13, 14]. Internal foot muscles, tendons, arteries, and nerves are arranged in four layers beneath the plantar aponeurosis. The superficial fascia was scraped off with a dull scalpel blade. A longitudinal incision was made in the plantar aponeurosis using a sharp blade. The thickness of the plantar aponeurosis is about 4 mm. As a result, it did not cut too deeply [15]. The plantar aponeurosis was then cut transversely. The muscles that make up the first layer of the sole’s muscles are the flexor digitorum brevis, abductor hallucis, and abductor digiti minimi [16]. In the distal third of the foot, the common and proper plantar digital nerves (branches of the medial and lateral plantar nerves) were visible. The common and proper digital nerves lie between the tendons just identified.
Dorsum of the foot and anterior and lateral compartments of the right leg
Due to the absence of deep anatomical inversions in the anterior compartment of the leg and on the dorsum of the foot, the right leg was dissected similar to the left leg [13]. The lateral compartment of the leg includes two muscles: Fibularis longus and fibularis brevis. Superficial fibular nerve is the nerve of lateral compartment. We dissected the fibularis longus and fibularis brevis muscles. The superficial peroneal nerve was located along the crural fascia at the mid-calf level. After being traced proximally, the tendons of the fibularis brevis and fibularis longus muscles were located beneath the superior and inferior fibular retinaculum.
The right foot plantar region was also dissected based on the steps similar to the left foot. The first layer muscles, including the abductor halluces, abductor digiti minimi, and flexor digitorum brevis were removed to expose the second layer of the sole including lumbricals and quadratus plantae.
Posterior compartment of the left leg
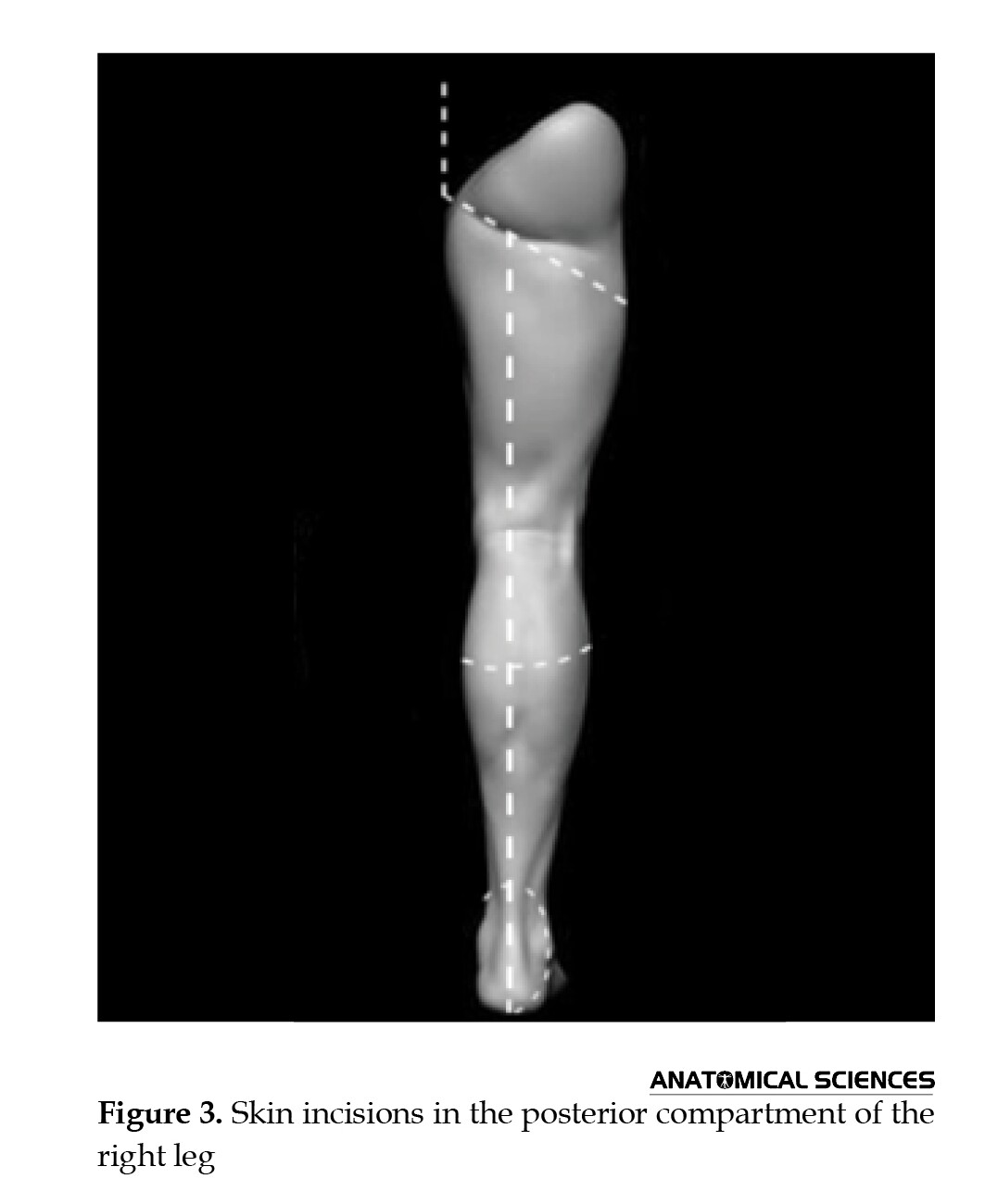
The muscles of the posterior compartment of the leg are separated into superficial and deep groups by a transverse intermuscular septum [17]. The plantaris, soleus, and gastrocnemius are the three muscles that together make up the superficial posterior group. Flexing the foot is the collective function of the muscles. The tibialis posterior, flexor hallucis longus, flexor digitorum longus, and popliteus are the four muscles that make up the deep posterior group. These muscles were revealed by the reflection of the superficial posterior group’s muscles (Figure 3).
The crural fascia was incised from the calcaneus to the popliteal fossa, opening the access to the posterior compartment of the leg. The gastrocnemius, soleus, and plantaris muscles were then identified and dissected. The tibial nerve and posterior tibial artery were followed through the popliteal fossa. The deep muscle group, including flexor digitorum longus, flexor hallucis longus, and tibialis posterior was examined.
The posterior tibial artery and tibial nerve were followed proximally by the probe [18]. At the inferior boundary of the popliteus muscle, the popliteal artery was shown to split into the anterior and posterior tibial arteries. The popliteal arteries and nerve were visible, and the contents of the popliteal fossa were laterally displaced. The popliteal artery’s branches were identified after it was traced to the leg’s posterior part. Additionally, the origin of the fibular artery was observed, and the posterior tibial artery was followed proximally. The posterior part of the leg and its many muscle branches were identified, and the tibial nerve was traced into the popliteal fossa.
Posterior compartment of the right leg
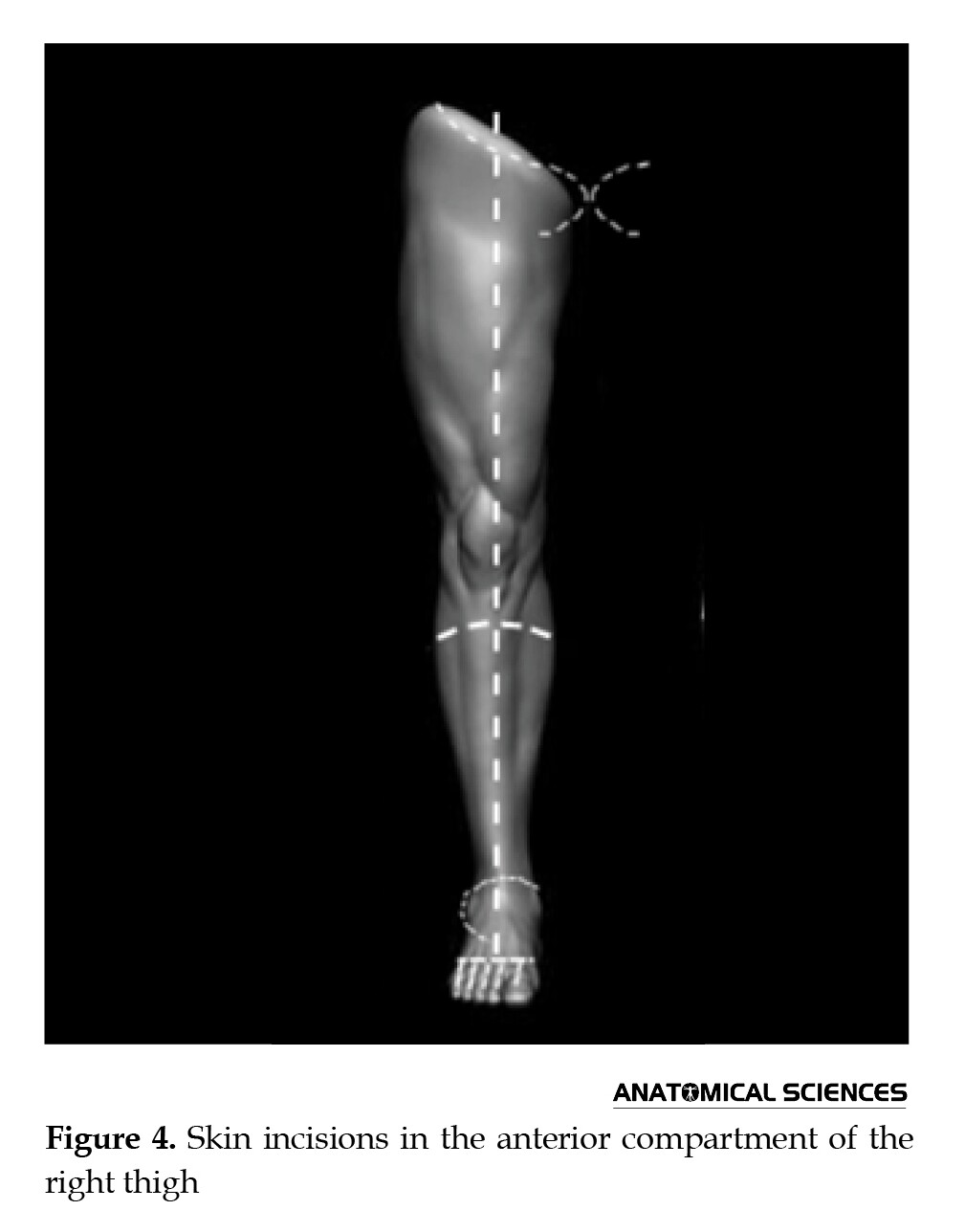
The posterior compartment of the right leg was dissected similarly to that of the left leg. The superficial muscles including the gastrocnemius, soleus and plantaris were removed to expose the deeper layer including tibialis posterior, flexor digitorum longus and flexor hallucis longus muscles and posterior tibial artery and tibial nerve (Figure 4).
Anterior compartment of the left thigh
In order to form the three fascial compartments of the thigh, the fascia lata is joined to the femur by intermuscular septa. The rectus femoris, vastus medialis, vastus intermedius, vastus lateralis, and sartorius are the five muscles that make up the anterior compartment of the thigh [19]. These muscles were identified and dissected. The femoral triangle was exposed, revealing the femoral artery, vein, and nerve. The adductor canal was opened to see the saphenous nerve and femoral vessels. The femoral triangle was examined by opening the anterior aspect of the superior fascia lata. The contents of the dissected femoral triangle were followed distally. They dissected the adductor canal. Any superficial fascia remnants that were still present on the fascia lata’s anterior surface between the knee and the inguinal ligament were eliminated. The great saphenous vein was followed and the connective tissue surrounding the great saphenous vein was dissected. After examining the femoral triangle, the femoral nerve, femoral artery, femoral vein, and some of their branches were seen, along with the femoral sheath. The femoral nerve was visible at the floor of the femoral triangle, lateral to the femoral artery. The femoral nerve was followed inferiorly and was found to divide into numerous branches.
The sartorius muscle and the deep fascia were separated by fingers [20]. Laterally retracting the sartorius muscle allowed for the examination of its blood and nerve supply as well as the identification of its superior and inferior attachments. The femoral vessels were enclosed in a connective tissue sheath posterior to the sartorius muscle [21]. The adductor canal is this sheath of connective tissue. The nerve to the vastus medialis and the saphenous nerve were seen in the adductor canal. The rectus femoris muscle was cut in the middle and its halves were turned up and down.
Anterior compartment of the left thigh
The anterior compartment of the right thigh was dissected similarly to that of the left thigh. The superficial muscles including sartorius and rectus femoris were removed to expose the adductor canal and underlying vastus muscles, particularly the vastus intermedius.
Posterior compartment of the left thigh
We made skin incisions in the posterior compartment of the left thigh according to Figure 5.
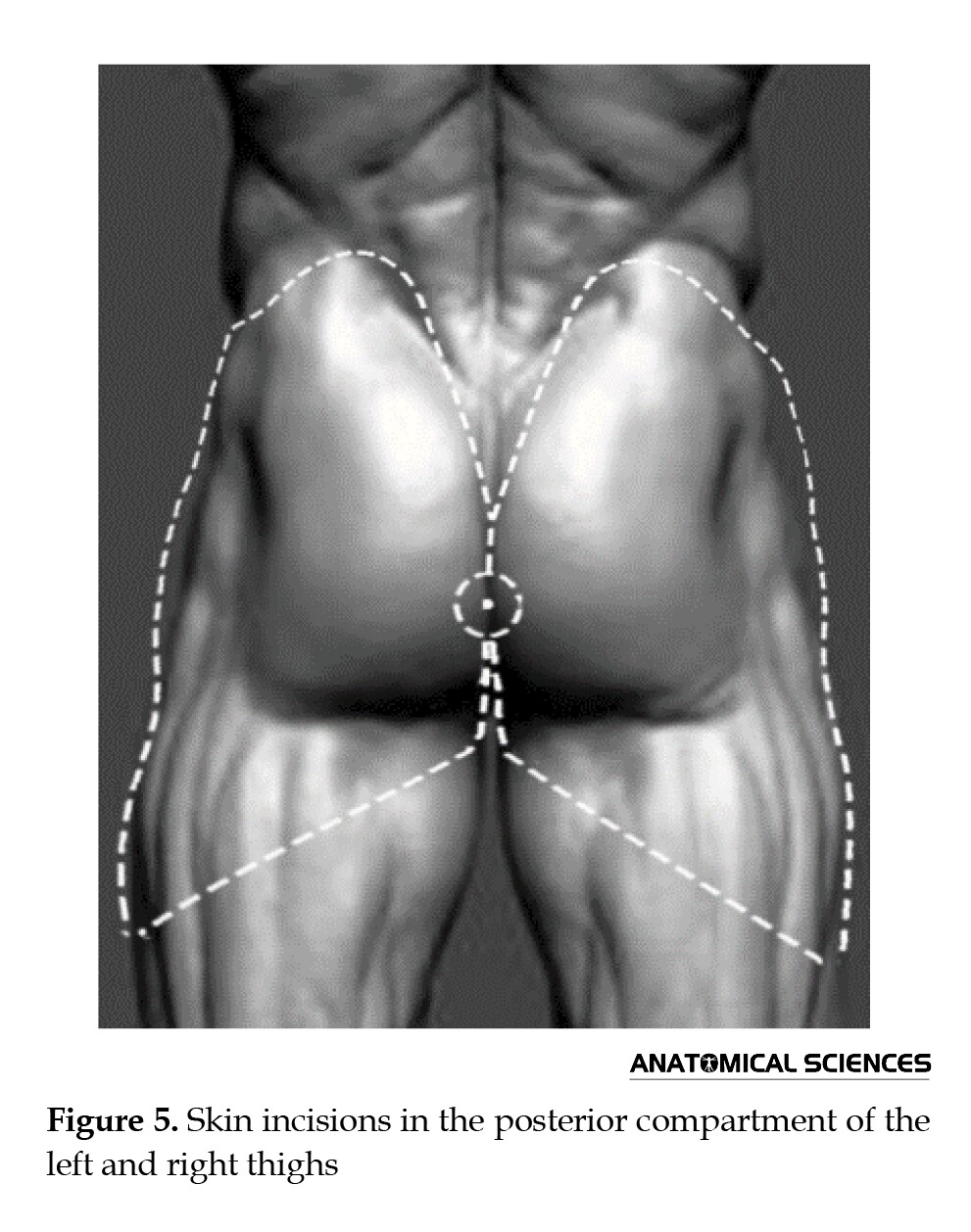
The biceps femoris, semitendinosus, and semimembranosus form the posterior compartment of the thigh [22]. The gluteus maximus muscle was fully exposed when the fascia lata was incised with scissors, starting from the level of the muscle and down to the knee [23]. Blunt dissection was used to explore the sciatic nerve and the nerve was followed distally [24]. In order to reveal the short head of the biceps femoris muscle, the long head was pushed laterally. The semitendinosus muscle is located on the medial side of the thigh. The semitendinosus and semimembranosus were separated by fingers. From the back of the thigh to the back of the knee, the sciatic nerve was also traced.
The common peroneal nerve was traced along the upper lateral margin of the popliteal fossa by blunt dissection. The medial and lateral heads of the gastrocnemius muscle were visible when the popliteal fascia remnants were cut away. The tibial nerve was then extracted from the loose connective tissue around it using the fingers. The index finger was positioned between the gastrocnemius muscle’s two ventricles, inferior to the popliteal fossa. The structures that enter the lower leg through the popliteal fossa were made visible by separating the muscle ventricles. Deep to the tibial nerve, the popliteal artery and vein were located [25]. The sheath was cut open with scissors. Lastly, the popliteal vein and artery were separated using a probe.
Posterior compartment of the right thigh
The posterior compartment of the right thigh was dissected similarly to that of the left side (Figure 5). The superficial muscles including biceps femoris, semitendinosus and semimembranosus were reflected to expose the underlying anatomical structures such as the sciatic nerve, profunda femoris artery and associated vascular and neural components.
Left gluteal region
The gluteal region’s fat and superficial fascia were excised. To reveal the muscles beneath the gluteus maximus, it was delineated and laterally removed. The surface of the fascia lata in the gluteal area was cleared of the superficial fascia, led to the identification of the gluteus maximus muscle. The superficial fascia in the inferior part of this muscle was also removed.
Right gluteal region
By removing the gluteus maximus, the deeper muscles of the right gluteal region—including the gluteus medius, gluteus minimus, and piriformis—were revealed. When the piriformis was completely dissected, it was found that the neurovascular structures that emerged beneath it were sciatic nerve, superior and inferior gluteal arteries, and nerves.
Results
The novel dissection method proposed in this study, utilizing a distal-to-proximal approach, proved effective in preserving the delicate anatomical structures of the lower limb. This technique mitigated the rapid desiccation typically encountered in traditional proximal-to-distal dissections, ensuring the integrity of tissues for plastination. The comparative dissection of the left and right limbs provided a unique educational opportunity. The left limb, with its superficial muscles intact, allowed for the study of surface anatomy, while the right limb, with superficial muscles removed, revealed deeper structures, including vessels, nerves, and deep muscles. This side-by-side comparison enhanced the understanding of spatial relationships and complex anatomical arrangements. The plastinated specimens produced using this method exhibited excellent preservation of tissue architecture and color, closely resembling living tissue. This method also successfully addressed the limitations of the traditional plastination method, which often results in rigid, inflexible specimens that lack the natural feel of living tissue.
Discussion
The distal-to-proximal dissection approach is a significant shift from traditional methods [26]. By beginning the dissection at the distal extremities, we were able to address the challenge of rapid desiccation in these areas [27]. This approach ensured that the tissues remained pliable and well-preserved throughout the dissection process, facilitating the subsequent plastination procedure.
The comparative dissection technique, utilizing both limbs of the cadaver, offered a comprehensive learning experience [28]. By preserving the superficial muscles on one limb and removing them on the contralateral limb, medical students can gain a deeper understanding of both surface and deep anatomy [29]. This approach also highlights the relationships between different anatomical structures and their functional significance.
The plastination method employed in this study resulted in specimens that closely resembled living tissue in terms of color and texture [30]. This is crucial for medical education, as it allows medical students to study anatomy in a realistic and engaging manner [31]. Additionally, the plastinated specimens are durable and odorless, making them ideal for long-term use in teaching and research.
This novel dissection and plastination methods have the potential to enhance medical education by providing high-quality anatomical specimens that are both informative and engaging [32]. The technique addresses the limitations of traditional methods and offers a valuable tool for teaching and research in anatomy.
Conclusion
The proposed novel dissection protocol offers an effective way to showcase both the superficial and deep structures of the lower limbs in a single, plastinated specimen. This approach not only helps with the preservation of anatomical details but also offers a valuable comparative learning tool for medical students.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
References
Plastination, pioneered by Gunther von Hagens in 1977, is a technique that preserves biological tissues while maintaining anatomical accuracy [1]. This method has revolutionized medical education by offering long-lasting odorless specimens that resemble living tissues [2]. However, one limitation of plastination is that, after final curing, the resulting specimen becomes rigid and non-flexible, with a plastic-like consistency [3].
Understanding the anatomical structure and function of the lower limbs, including muscles, nerves, and vessels, is crucial for medical students [4]. In this study, we aim to propose a novel dissection approach for lower limb plastination, optimizing tissue preservation and educational value while maintaining anatomical integrity. We dissect the left and right limbs differently. The left limb is dissected, preserving its superficial muscles for standard anatomical study [5], while the superficial muscles of the right limb are removed, exposing deep anatomical structures such as vessels, nerves, and deep muscles. This approach allows for a comparative study of both surface and deep layers in a single specimen.
Materials and Methods
Dissection protocol
The proposed dissection protocol is different from the traditional proximal-to-distal approach. The cadaver was embalmed with a strong fixative and kept moist to prevent desiccation [6]. To optimize plastination, we performed dissection in a distal-to-proximal direction, preserving anatomical structures while minimizing tissue damage [7]. The skin was removed gradually, ensuring that the subcutaneous fat (which can delay plastination) was carefully excised. We dissected the superficial muscles, vessels, and nerves in one limb, while they were removed in the other limb to expose the deep structures. This technique allows for a comprehensive analysis of anatomical layers.
Skin removal
The first step in the dissection process was the skin excision. Directly beneath the skin, there are different layers of subcutaneous tissue, known as superficial fascia. This layer contains cutaneous nerves, adipose tissue, and superficial vascular structures [8]. We had to remove the skin with subcutaneous fat.
The skin was removed using toothed forceps and the scalpel blade [1]. The scalpel blade should be directed deep into the skin to cut the collagen fibers. Cutaneous nerves and superficial veins were dissected and the fat was eliminated to better see the deep fascia. For this purpose, in one lower limb, we dissected the superficial muscles with nerves and vessels, while removing them in the other limb to determine the deep muscles, vessels, and nerves.
Dorsum of the foot and anterior and lateral compartments of the left leg
The dorsum of the foot, behind the toes, was incised, followed by more cuts along the dorsal midline of each toe to the proximal end of the nail [9]. Finally, skin was picked up from the dorsum of the foot in the lateral and medial directions. The anterior compartment, consisting of extensor hallucis longus, tibialis anterior, fibularis tertius, and extensor digitorum longus, was dissected. The deep fibular nerve and anterior tibial artery were traced distally. The anatomical path of the dorsalis pedis artery was determined by following it onto the foot [10]. The superior extensor retinaculum is the level at which the anterior tibial artery is located. A distal direction of the anterior tibial artery was then seen. The probe was used to clean the artery. Along this path, it was observed that the anterior tibial artery joins the deep fibular nerve just below the knee. The deep fibular nerve was followed proximally and confirmed to be a branch of the common fibular nerve (Figure 1).
On the foot’s dorsum, the extensor hallucis brevis and extensor digitorum brevis muscles are located beneath the tendons of the extensor digitorum longus muscle. The dorsalis pedis artery is also seen on the dorsum [11]. It runs along the lateral side of the extensor hallucis longus tendon near the ankle in the distal part of the leg. On the leg’s anterior compartment, the superficial fascia remnants were removed [12]. In order to make the crural fascia visible, we identified the anterior surface of the ankle’s superior and inferior extensor retinacula. The tibialis anterior and extensor digitorum longus muscles were separated by fingers. Between the two muscles, the anterior tibial artery was traced proximally.
The plantar region of the left foot was also dissected (Figure 2). The foot has a longitudinal arch. The calcaneus (located posteriorly) and the heads of the five metatarsals (located anteriorly) are among the weight-bearing points in the foot [13, 14]. Internal foot muscles, tendons, arteries, and nerves are arranged in four layers beneath the plantar aponeurosis. The superficial fascia was scraped off with a dull scalpel blade. A longitudinal incision was made in the plantar aponeurosis using a sharp blade. The thickness of the plantar aponeurosis is about 4 mm. As a result, it did not cut too deeply [15]. The plantar aponeurosis was then cut transversely. The muscles that make up the first layer of the sole’s muscles are the flexor digitorum brevis, abductor hallucis, and abductor digiti minimi [16]. In the distal third of the foot, the common and proper plantar digital nerves (branches of the medial and lateral plantar nerves) were visible. The common and proper digital nerves lie between the tendons just identified.
Dorsum of the foot and anterior and lateral compartments of the right leg
Due to the absence of deep anatomical inversions in the anterior compartment of the leg and on the dorsum of the foot, the right leg was dissected similar to the left leg [13]. The lateral compartment of the leg includes two muscles: Fibularis longus and fibularis brevis. Superficial fibular nerve is the nerve of lateral compartment. We dissected the fibularis longus and fibularis brevis muscles. The superficial peroneal nerve was located along the crural fascia at the mid-calf level. After being traced proximally, the tendons of the fibularis brevis and fibularis longus muscles were located beneath the superior and inferior fibular retinaculum.
The right foot plantar region was also dissected based on the steps similar to the left foot. The first layer muscles, including the abductor halluces, abductor digiti minimi, and flexor digitorum brevis were removed to expose the second layer of the sole including lumbricals and quadratus plantae.
Posterior compartment of the left leg
The muscles of the posterior compartment of the leg are separated into superficial and deep groups by a transverse intermuscular septum [17]. The plantaris, soleus, and gastrocnemius are the three muscles that together make up the superficial posterior group. Flexing the foot is the collective function of the muscles. The tibialis posterior, flexor hallucis longus, flexor digitorum longus, and popliteus are the four muscles that make up the deep posterior group. These muscles were revealed by the reflection of the superficial posterior group’s muscles (Figure 3).
The crural fascia was incised from the calcaneus to the popliteal fossa, opening the access to the posterior compartment of the leg. The gastrocnemius, soleus, and plantaris muscles were then identified and dissected. The tibial nerve and posterior tibial artery were followed through the popliteal fossa. The deep muscle group, including flexor digitorum longus, flexor hallucis longus, and tibialis posterior was examined.
The posterior tibial artery and tibial nerve were followed proximally by the probe [18]. At the inferior boundary of the popliteus muscle, the popliteal artery was shown to split into the anterior and posterior tibial arteries. The popliteal arteries and nerve were visible, and the contents of the popliteal fossa were laterally displaced. The popliteal artery’s branches were identified after it was traced to the leg’s posterior part. Additionally, the origin of the fibular artery was observed, and the posterior tibial artery was followed proximally. The posterior part of the leg and its many muscle branches were identified, and the tibial nerve was traced into the popliteal fossa.
Posterior compartment of the right leg
The posterior compartment of the right leg was dissected similarly to that of the left leg. The superficial muscles including the gastrocnemius, soleus and plantaris were removed to expose the deeper layer including tibialis posterior, flexor digitorum longus and flexor hallucis longus muscles and posterior tibial artery and tibial nerve (Figure 4).
Anterior compartment of the left thigh
In order to form the three fascial compartments of the thigh, the fascia lata is joined to the femur by intermuscular septa. The rectus femoris, vastus medialis, vastus intermedius, vastus lateralis, and sartorius are the five muscles that make up the anterior compartment of the thigh [19]. These muscles were identified and dissected. The femoral triangle was exposed, revealing the femoral artery, vein, and nerve. The adductor canal was opened to see the saphenous nerve and femoral vessels. The femoral triangle was examined by opening the anterior aspect of the superior fascia lata. The contents of the dissected femoral triangle were followed distally. They dissected the adductor canal. Any superficial fascia remnants that were still present on the fascia lata’s anterior surface between the knee and the inguinal ligament were eliminated. The great saphenous vein was followed and the connective tissue surrounding the great saphenous vein was dissected. After examining the femoral triangle, the femoral nerve, femoral artery, femoral vein, and some of their branches were seen, along with the femoral sheath. The femoral nerve was visible at the floor of the femoral triangle, lateral to the femoral artery. The femoral nerve was followed inferiorly and was found to divide into numerous branches.
The sartorius muscle and the deep fascia were separated by fingers [20]. Laterally retracting the sartorius muscle allowed for the examination of its blood and nerve supply as well as the identification of its superior and inferior attachments. The femoral vessels were enclosed in a connective tissue sheath posterior to the sartorius muscle [21]. The adductor canal is this sheath of connective tissue. The nerve to the vastus medialis and the saphenous nerve were seen in the adductor canal. The rectus femoris muscle was cut in the middle and its halves were turned up and down.
Anterior compartment of the left thigh
The anterior compartment of the right thigh was dissected similarly to that of the left thigh. The superficial muscles including sartorius and rectus femoris were removed to expose the adductor canal and underlying vastus muscles, particularly the vastus intermedius.
Posterior compartment of the left thigh
We made skin incisions in the posterior compartment of the left thigh according to Figure 5.
The biceps femoris, semitendinosus, and semimembranosus form the posterior compartment of the thigh [22]. The gluteus maximus muscle was fully exposed when the fascia lata was incised with scissors, starting from the level of the muscle and down to the knee [23]. Blunt dissection was used to explore the sciatic nerve and the nerve was followed distally [24]. In order to reveal the short head of the biceps femoris muscle, the long head was pushed laterally. The semitendinosus muscle is located on the medial side of the thigh. The semitendinosus and semimembranosus were separated by fingers. From the back of the thigh to the back of the knee, the sciatic nerve was also traced.
The common peroneal nerve was traced along the upper lateral margin of the popliteal fossa by blunt dissection. The medial and lateral heads of the gastrocnemius muscle were visible when the popliteal fascia remnants were cut away. The tibial nerve was then extracted from the loose connective tissue around it using the fingers. The index finger was positioned between the gastrocnemius muscle’s two ventricles, inferior to the popliteal fossa. The structures that enter the lower leg through the popliteal fossa were made visible by separating the muscle ventricles. Deep to the tibial nerve, the popliteal artery and vein were located [25]. The sheath was cut open with scissors. Lastly, the popliteal vein and artery were separated using a probe.
Posterior compartment of the right thigh
The posterior compartment of the right thigh was dissected similarly to that of the left side (Figure 5). The superficial muscles including biceps femoris, semitendinosus and semimembranosus were reflected to expose the underlying anatomical structures such as the sciatic nerve, profunda femoris artery and associated vascular and neural components.
Left gluteal region
The gluteal region’s fat and superficial fascia were excised. To reveal the muscles beneath the gluteus maximus, it was delineated and laterally removed. The surface of the fascia lata in the gluteal area was cleared of the superficial fascia, led to the identification of the gluteus maximus muscle. The superficial fascia in the inferior part of this muscle was also removed.
Right gluteal region
By removing the gluteus maximus, the deeper muscles of the right gluteal region—including the gluteus medius, gluteus minimus, and piriformis—were revealed. When the piriformis was completely dissected, it was found that the neurovascular structures that emerged beneath it were sciatic nerve, superior and inferior gluteal arteries, and nerves.
Results
The novel dissection method proposed in this study, utilizing a distal-to-proximal approach, proved effective in preserving the delicate anatomical structures of the lower limb. This technique mitigated the rapid desiccation typically encountered in traditional proximal-to-distal dissections, ensuring the integrity of tissues for plastination. The comparative dissection of the left and right limbs provided a unique educational opportunity. The left limb, with its superficial muscles intact, allowed for the study of surface anatomy, while the right limb, with superficial muscles removed, revealed deeper structures, including vessels, nerves, and deep muscles. This side-by-side comparison enhanced the understanding of spatial relationships and complex anatomical arrangements. The plastinated specimens produced using this method exhibited excellent preservation of tissue architecture and color, closely resembling living tissue. This method also successfully addressed the limitations of the traditional plastination method, which often results in rigid, inflexible specimens that lack the natural feel of living tissue.
Discussion
The distal-to-proximal dissection approach is a significant shift from traditional methods [26]. By beginning the dissection at the distal extremities, we were able to address the challenge of rapid desiccation in these areas [27]. This approach ensured that the tissues remained pliable and well-preserved throughout the dissection process, facilitating the subsequent plastination procedure.
The comparative dissection technique, utilizing both limbs of the cadaver, offered a comprehensive learning experience [28]. By preserving the superficial muscles on one limb and removing them on the contralateral limb, medical students can gain a deeper understanding of both surface and deep anatomy [29]. This approach also highlights the relationships between different anatomical structures and their functional significance.
The plastination method employed in this study resulted in specimens that closely resembled living tissue in terms of color and texture [30]. This is crucial for medical education, as it allows medical students to study anatomy in a realistic and engaging manner [31]. Additionally, the plastinated specimens are durable and odorless, making them ideal for long-term use in teaching and research.
This novel dissection and plastination methods have the potential to enhance medical education by providing high-quality anatomical specimens that are both informative and engaging [32]. The technique addresses the limitations of traditional methods and offers a valuable tool for teaching and research in anatomy.
Conclusion
The proposed novel dissection protocol offers an effective way to showcase both the superficial and deep structures of the lower limbs in a single, plastinated specimen. This approach not only helps with the preservation of anatomical details but also offers a valuable comparative learning tool for medical students.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
References
- Von Hagens G. Impregnation of soft biological specimens with thermosetting resins and elastomers. Anatomical Record. 1979; 194(2):247-55. [DOI:10.1002/ar.1091940206] [PMID]
- Von Hagens, G. Plastination of whole animal bodies and organs. Anatomical Record. 1986; 216(1), 47-57.
- Von Hagens G, Tiedemann K, Kriz W. The current potential of plastination. Anatomy and Embryology. 1987; 175(4):411-21. [DOI:10.1007/BF00309677] [PMID]
- Latorre RM, García-Sanz MP, Moreno M, Hernández F, Gil F, López O, Ayala MD, et al. How useful is plastination in learning anatomy?. Journal of veterinary Medical Education. 2007; 34(2):172-6. [Link]
- Henry RW, Johnson TW. Plastination: A review of current techniques and applications. Journal of Veterinary Medical Education. 2012; 39(2):163-76.
- Ahmadi M, Tehrani M, Shakeri S. Plastination: A novel method in anatomical studies. Journal of Anatomy Society of India. 2016; 65(1):1-8.
- Diogo R, Abdala V, Wood B. Plastination of whole skeletons: a new method for preserving and displaying large specimens. Journal of Anatomy. 2018; 232(5):856-63.
- Drake LD, Vogl AW, Mitchell AWM. Gray's Atlas of Anatomy. Amsterdam: Elsevier Health Sciences; 2020. [Link]
- Moore KL, Dalley AF, Agur AMR. Clinically oriented anatomy. Philadelphia: Lippincott Williams & Wilkins; 2017. [Link]
- Gilroy AM, MacPherson BR, Ross LM. Atlas of anatomy. Teningen: Thieme; 2020. [Link]
- Standring S. Gray’s anatomy: The anatomical basis of clinical practice. Amesterdam: Elsevier Health Sciences; 2020.
- Tank PW. Grant’s dissector. Philadelphia: Lippincott Williams & Wilkins; 2013. [Link]
- Azer SA, Eizenberg N, Puddey IB. Students’ perceptions of learning anatomy by prosection or dissection. BMC Medical Education. 2013; 13(1)1-10.
- Hansen JT (2018). Netter’s clinical anatomy. Amesterdam: Elsevier Health Sciences. [Link]
- Papa V, Vaccarezza M. Teaching anatomy in the XXI century: New aspects and pitfalls. ScientificWorld Journal of Anatomy. 2013:2013:310348. [DOI: 10.1155/2013/310348] [PMID]
- Turney BW. Anatomy in a modern medical curriculum. Annals of the Royal College of Surgeons of England. 2007; 89(2):104-7. [DOI:10.1308/003588407X168244] [PMID]
- McLachlan JC, Patten D. Anatomy teaching: ghosts of the past, present and future. Medical Education. 2006; 40(3):243-53. [DOI:10.1111/j.1365-2929.2006.02401.x] [PMID]
- Kierzenkowski B, Ravnan SL. The use of plastinated specimens in medical education: A review of the literature. Anatomical Sciences Education. 2018; 11(6):639-46.
- Evans DJ, Watt DJ. Plastinated specimens: A valuable resource for teaching and learning anatomy. Anatomical Sciences Education. 2013; 6(4):263-71.
- Choi BY, Kim DY, Kwak HH. The effectiveness of plastinated specimens for teaching and learning anatomy: a systematic review. Anatomical Sciences Education. 2019; 12(6):668-78.
- Platzer W. Color atlas of human anatomy. Thieme. 2004.
- Agur AMR, Dalley AF. Grant’s atlas of anatomy. Alphen aan den Rijn: Wolters Kluwer; 2024. [Link]
- Rohen JW, Yokochi C, Lütjen-Drecoll E. Color atlas of anatomy: A photographic study of the human body. Alphen aan den Rijn; Wolters Kluwer Health/Lippincott Williams & Wilkins; 2011.
- Moore KL, Agur AMR, Dalley AF. Essential clinical anatomy. Alphen aan den Rijn: Lippincott Williams & Wilkins; 2015. [Link]
- Dutton, M. Orthopaedic examination, evaluation, and intervention. New York: McGraw-Hill Education; 2012. [Link]
- Magee DJ. Orthopedic physical assessment. Amesterdam: Elsevier Health Sciences; 2014. [Link]
- Steinberg BD, Plunkett BP. A new approach to the dissection of the human cadaver: the use of plastinated specimens. Clinical Anatomy. 2009; 22(1):122-7.
- Goyal RK, Gupta P. A new technique for the dissection of the human cadaver: The use of plastinated specimens. Journal of Anatomy Society of India. 2011; 60(1):1-4.
- Hammer N, Löffler S, Feja C. Plastination of the human body: a new approach to the dissection of the human cadaver. Clinical Anatomy. 2012; 25(1):127-33.
- Waldman SD. Atlas of common pain syndromes. Amesterdam: Elsevier Health Sciences; 2011. [Link]
- Travell JG, Simons D. Myofascial pain and dysfunction: The trigger point manual. Philadelphia: Lippincott Williams & Wilkins; 1992. [Link]
- Bordoni B, Zanier E. Anatomic connections of the diaphragm: influence of respiration on the body system. Journal of Multidisciplinary Healthcare. 2013; 6:281-91. [DOI: 10.2147/JMDH.S45443] [PMID]
Type of Study: Original |
Subject:
Plastination
Received: 2025/02/25 | Accepted: 2025/03/8 | Published: 2023/08/30
Received: 2025/02/25 | Accepted: 2025/03/8 | Published: 2023/08/30
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
