Mon, Jul 20, 2026
Volume 19, Issue 1 (Winter & Spring 2022)
ASJ 2022, 19(1): 1-10 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Bakhshi Kashi M, Behnejad M, Loghman A H, Zamani-Badi T, Nikzad H. Study of Median Nerve Variations and Its Clinical Implications at the Distal Part of Upper Limb: A Review. ASJ 2022; 19 (1) :1-10
URL: http://anatomyjournal.ir/article-1-189-en.html
URL: http://anatomyjournal.ir/article-1-189-en.html
Mohsen Bakhshi Kashi1 
 , Milad Behnejad1 , Amir Hossein Loghman1 , Tayyebeh Zamani-Badi2 , Hossein Nikzad2
, Milad Behnejad1 , Amir Hossein Loghman1 , Tayyebeh Zamani-Badi2 , Hossein Nikzad2 
, Milad Behnejad1 , Amir Hossein Loghman1 , Tayyebeh Zamani-Badi2 , Hossein Nikzad2
1- School of Medicine, Kashan University of Medical Sciences, Kashan, Iran.
2- Anatomical Sciences Research Center, Kashan University of Medical Sciences, Kashan, Iran.
2- Anatomical Sciences Research Center, Kashan University of Medical Sciences, Kashan, Iran.
Full-Text [PDF 597 kb]
(1906 Downloads)
| Abstract (HTML) (4196 Views)
Full-Text: (3364 Views)
1. Introduction
Lateral (C5,6,7) and medial (C8, T1) cords of brachial plexus (BP) give two main median nerve (MN) roots uniting anterior to the axillary artery to form MN [1]. This formation pattern follows the BP embryological development basis in which the upper limb buds are included in the cervicothoracic segments (C5-T1) region and develop through the upper limb mesoderm and pierces it as ventral rami of the spinal cord [2].
After forming anterolaterally to the brachial artery, MN distally runs and crosses to the medial side of the brachial artery. Interestingly, branches supplying the elbow joint are reported as a single division of MN in the arm and axilla. The medial aspect of the brachial artery and heads of pronator teres are entrance and exit points that MN passes through them within the cubital fossa. Then MN runs between flexor digitorum superficialis and profondus to hand while passes deep to Palmaris longus and flexor retinaculum. The distal edge of the flexor retinaculum is the point at which the recurrent branch derives from the lateral side of the MN trunk supplying three Thenar muscles. Then, it runs around the flexor retinaculum. After passing between the flexor pollicis brevis and abductor pollicis brevis, its pathway ends in the medial edge of the opponens pollicis muscle, and then two main ramus derive from MN. The lateral ramus (first Common Digital Nerve [CDN]) supplies the thumb and lateral side of an index by two Proper Palmar Digital Nerves (PPDN), which the nerve to the radial side of the index innervates the first lumbrical muscle. The medial ramus divides into two (second and third) CDN supplying medial aspects of the index and adjacent sides of the middle digit and lateral side of the ring digit, and the second CDN supplies the second lumbrical muscle [1, 3].
Behnejad et al. [4] studied MN variations in the proximal part of the upper limbs. However, the complications involved in MN distal to cubital fossa are common and have clinical importance; for example, entrapment of MN in the carpal tunnel is the most common entrapment neuropathy in the clinical setting [5, 6, 7]. Still, anatomical variations from unremarkable abnormality to noticeable changes with diagnostic and therapeutic clinical importance can affect every part of the human body. MN variations also are common and are investigated and reported by many authors [8, 9, 10, 11, 12, 13, 14].
This survey aims to study median nerve variations and their clinical implications in the distal part of the upper limb to help surgeons, electrophysicians, and radiologists better know MN anatomy and anomaly to decrease iatrogenic mistakes.
2. Materials and Methods
This study is based on data published about MN variation from 1990 to 2020. Pubmed, Science Direct, and Google Scholar were researched to obtain relevant data by the following keywords: “Median nerve,” “Brachial plexus,” “Carpal tunnel,” and MeSH phrases made from the terms “Variation,” and “Cadaveric study.” We limited our research to dissection investigations. After downloading articles, we again searched associated references of pieces of literature to increase our data. Case reports, multiple cadaveric studies, and review articles were chosen for this study, and we didn’t apply any limitations. After reading the full text of all papers, we classified MN variations as reported in this paper.
3. Results
We categorized MN variations and coexistence anomalies into five groups as reported. Communication between the 4th common digital nerve of UN to the 3rd CDN of MN is the most common MN variation at the distal of the upper limb. The total numbers of cases with variation in the distribution of MN are 327 cases (Table 1).

4. Discussion
MN anatomy distal to cubital fossa doesn’t wholly match with related anatomy textbooks explanations and its different anatomy reported by many authors [8, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41]. The MN anomalies have spread spectrum in type and prevalence [8, 9, 10, 13, 37]. Notably, the prevalence of variation investigated in dissection studies is more common than in surgical observation, probably because of limitations on patient dissection [10, 13, 42, 43, 44]. We mention coexistence anomalies in the separation part because MN variation can be attributed to other coexistence variations disrupting normal MN development [9, 15, 32]. Variations in the distribution of MN were reported in 252 cases, including different types of variations. Of 327 patients, 113 can be categorized in one of Lanz’s classification groups (Tables 2, 3, 4 and 5).

However, the new variations compiled from cadaveric observations can be classified into five groups:
I) Variation in the distribution of MN in palm (Table 5)
II) Variation in MN innervation pattern (Table 5)
III) Communicating branches between MN and UN in the forearm (Table 6)
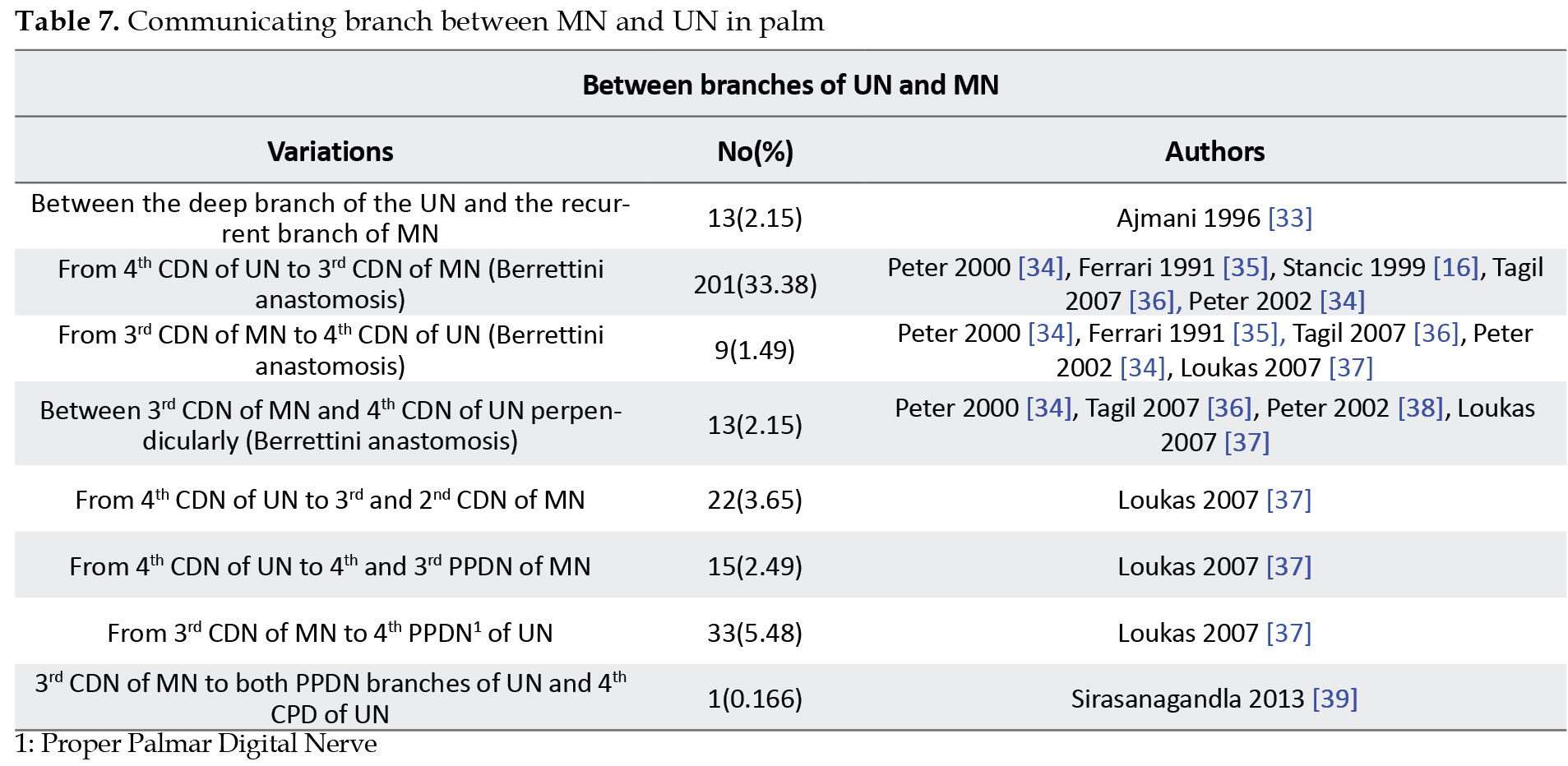
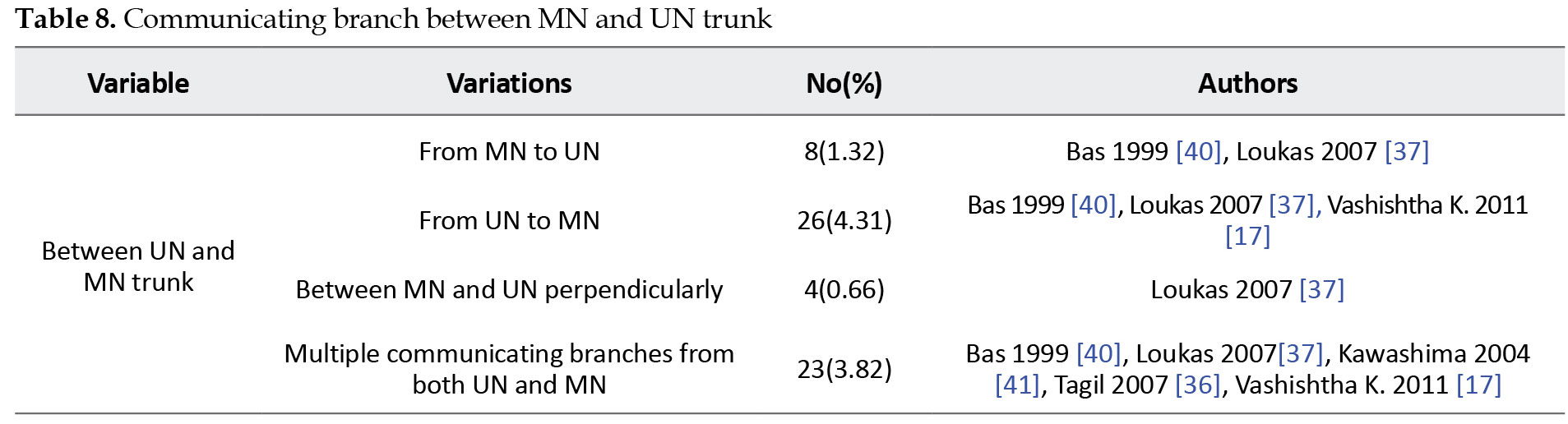
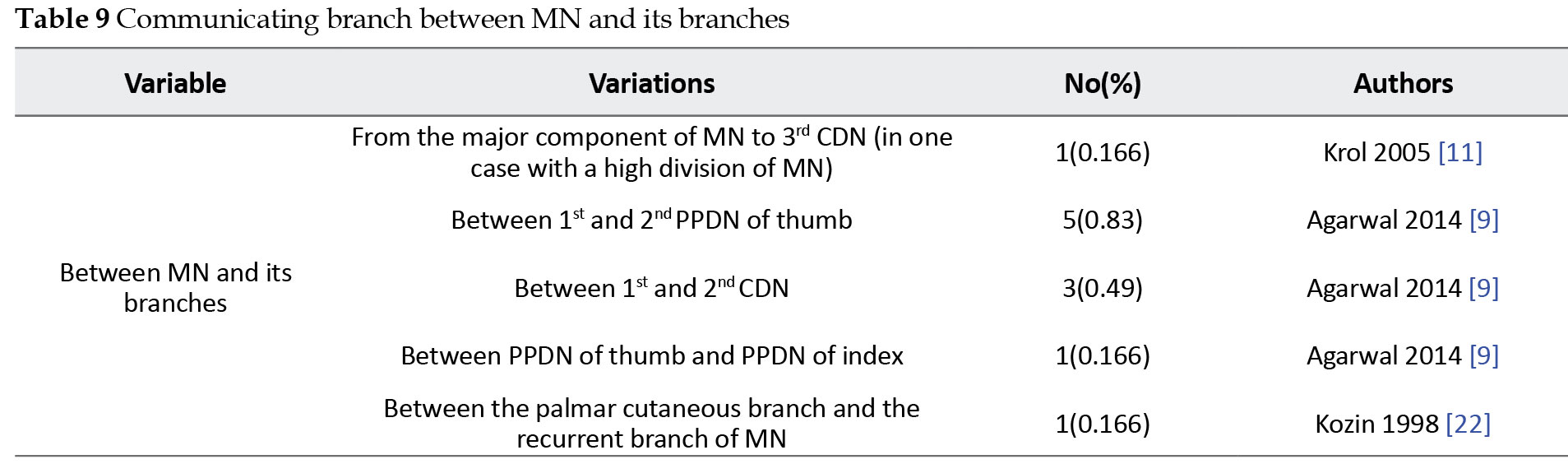
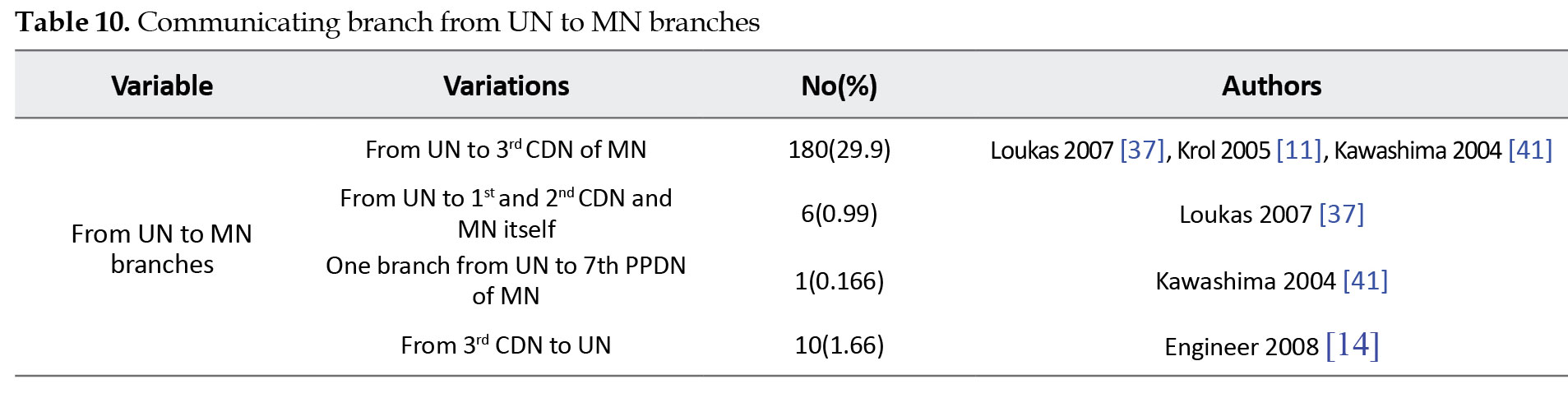
IV) Communicating branches between MN and UN in palm (Tables 7, 8, 9, 10 and 11)
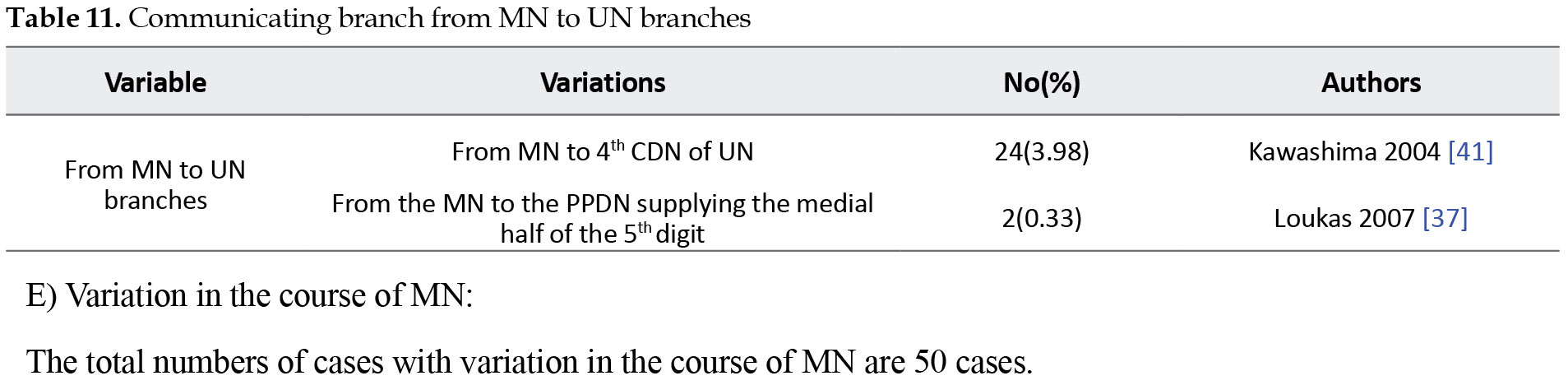
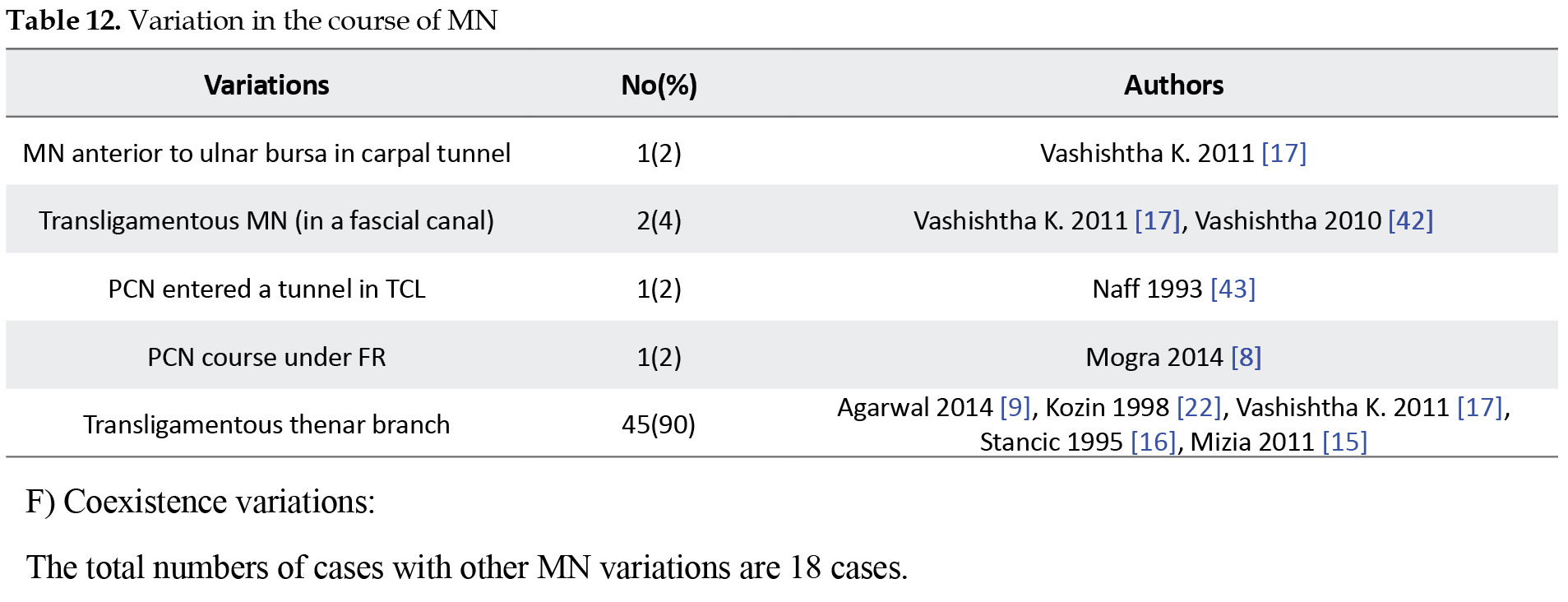
V) Variation in the course of MN (Table 12)
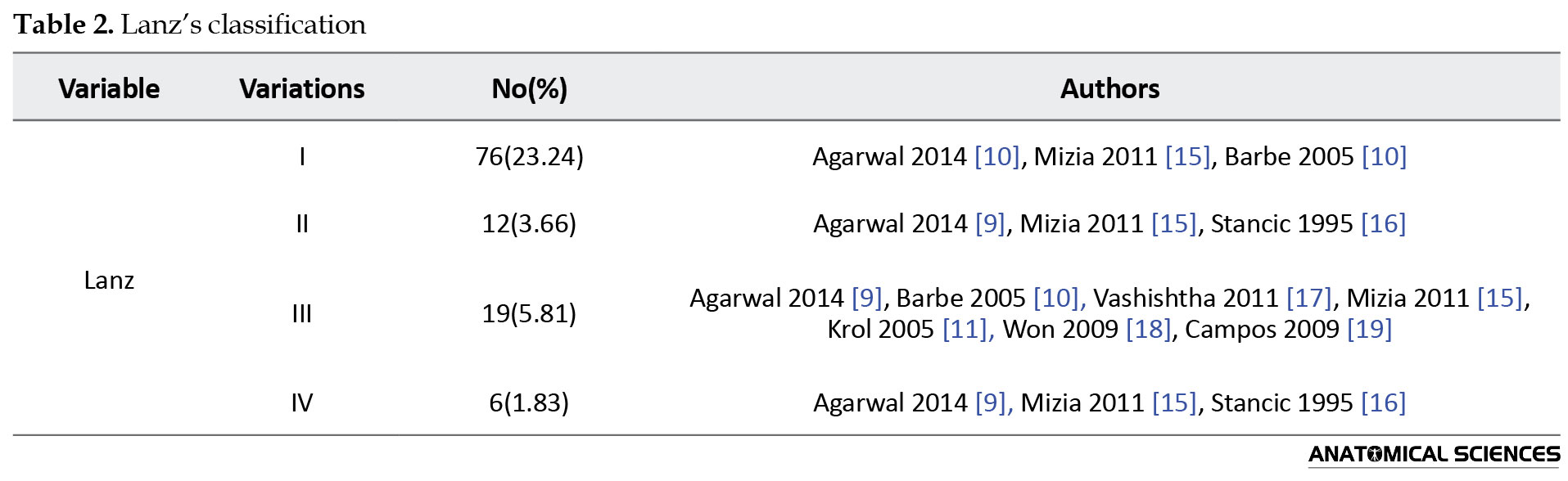
Lanz’s classification contains (Tables 2, 3 and 4):
I) Variation of thenar branch course
II) Accessory branches derived from MN at the distal of carpal tunnel
III) High division of MN
IV) Accessory branches derived from MN at the proximal part of carpal tunnel
The prevalence of MN variation described by Lanz’s groups (I-IV) were 46%, 7.5%, 2.9%, and 2.9%, respectively [13]. However, our study verifies the high prevalence of Lanz I, too.
Entrapment of MN beneath the flexor retinaculum presented by carpal tunnel syndrome, including some symptoms (such as numbness and weakness) and signs (such as Tinel sign and Phalen sign). These signs and symptoms can be alleviated by decompressing MN via endoscopic or open surgeries [45, 46, 47, 48]. Unfortunately, injury to the third common digital nerve (TCDN) is the most common post-carpal tunnel release operation complication [49]. Despite the clinical importance of the TCDN branching pattern, its variations had not been reported since Engineer et al. [14] classified variations of TCDN into three groups:
1) TCDN originates from MN proximal to the distal edge of the TCL
2) TCDN originates from MN distal to TCL but proximal to superficial palmar arch
3) TCDN originates from MN distal to TCL and superficial palmar arch
Notably, all TCDN variations may be vulnerable to damage by open carpal tunnel surgeries. Types 2 and 3 may potentially risk injury in endoscopy techniques. Despite visualization limitations, the Agee endoscopic surgery technique can preserve TCDN and its three types of variations from possible damage if done by a professional surgeon [14].
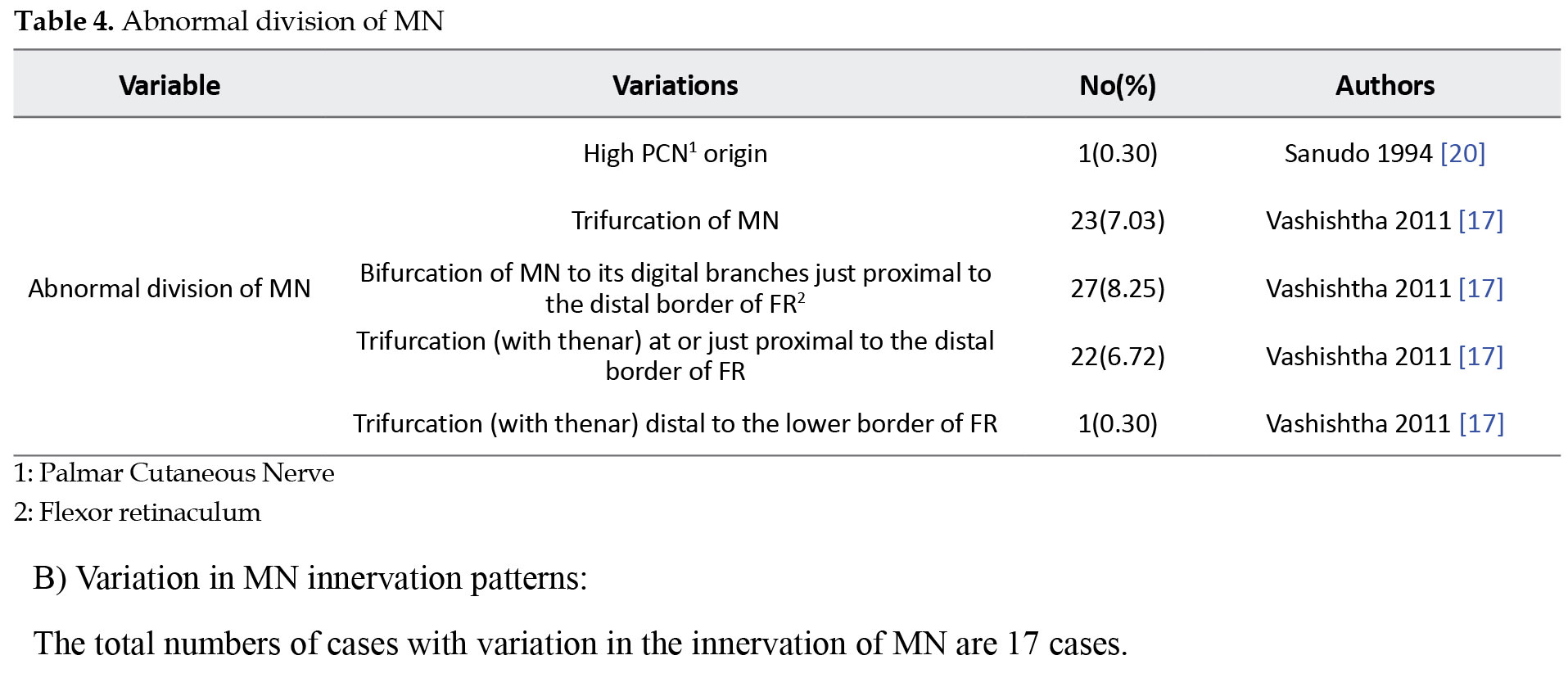
High bifurcation and trifurcation of MN are common variations of MN distribution [17]. Amadio documented high bifurcation MN in 9 cases in carpal tunnel decompression surgery [50]. Abnormal origination of recurrent branches is another variation of MN distribution, increasing the risk of MN injuries in carpal tunnel decompression [17].
Supplying all lumbricals from UN is highly associated with the presence of MGA in the forearm [23]. Originating the third lumbrical muscle nerve from MN is a rare variation reported by some authors [17, 51]. However, proximal UN injuries with incomplete clawed-hand must be considered as the presence of MGA [52]. Linell [53] reported one hand in which the UN supplied two sides of the ring finger and three hands in which the UN innervated the medial side of the middle finger. However, all variations associated with MN innervations patterns may disrupt post-trauma evaluations.
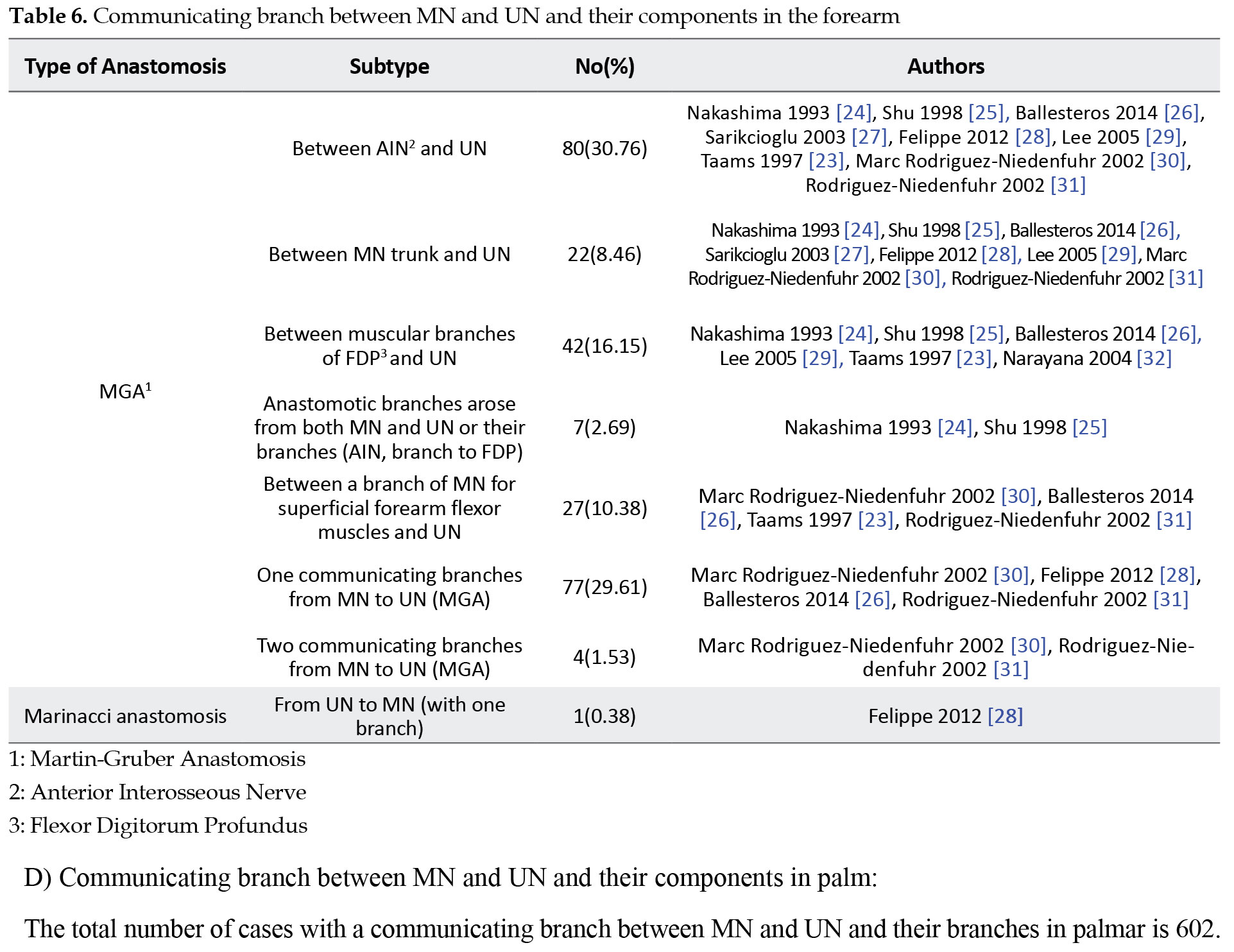
Martin-Gruber anastomosis was first described by Swedish anatomist Martin (1763) [54] and Gruber (1810) [55], is a connection between MN and UN in the forearm, and it can be classified into seven subtypes as documented in the previous part (Table 5). MGA has been seen in the primate’s elbows too. The MGA reveals a common trunk supplying the flexor compartment of the forearm in embryological life [56]. Examination of family members with MGA variations indicated some genetic features of this variation, and an Autosomal Dominant pattern was suggested for it [57]. Some hypotheses consider the role of chromosome 21 in this variation. Srinvasan and Rhodos [58] reported MGA bilaterally in fetuses carrying an extra 21 chromosomes (21 trisomies). Prevalence of MGA follows a difference statistically high prevalence of MGA was reported by Erdem et al. [59], Amoiridis [60], Lee et al. [29], and medium prevalence was reported by Shu et al. [25], and Nakashima [24] and low prevalence of this variation was documented by de Alemida et al. [61] and Prates et al. [62]. These different ranges can be explained by the different methodology used for studies and genetic variation between examined target populations [26]. Notably, MGA can change the clinical manifestations of patients suffering from pronator syndrome by changing muscle innervation patterns and sensory distribution [28, 63].
Marinacci anastomosis, called Martin-Gruber reverse anastomosis too, was first reported in a patient who presented with MN trauma, and despite forearm flexor muscle denervation, hand muscle function was normal [64]. However, communicating branch from UN to MN (Marinacci anastomosis) is a rare variation, and Kimura et al. [65] didn’t report any UN to MN communication in their electrophysiological examinations.
Palmar communication between MN and UN is the most common variation of MN and can be categorized into five subtypes as presented. Communicating branches often arose from UN to MN and were reported by some authors [23, 56, 57, 66]. However, the crucial role of these connections is in changing the pattern of sensory loss when MN or UN is compressed, which may lead to clinical mistakes [67].
Petro Berrettini [68] was the first man to paint the superficial palmar communication between UN and MN in the anatomy atlas. The Berrettini anastomosis can be categorized into three groups, as reported in the previous part (Table 4). However, some authors believed that Berretin anastomosis must be considered a normal anatomic discovery, and even in some papers, this anastomosis has been seen in all cases [69, 70].
Don Griot et al. [34] emphasized the advantage of Berretin anastomosis knowledge for surgeons performing carpal tunnel release, Dupuytren fasciotomy, and flexor tendons surgeries. Because of the high prevalence of UN and MN communications and their possible role in either diagnostic or therapeutic mistakes, some studies should be done to evaluate the relation of these variations and their potential clinical manifestation.
Subligamentous, Extraligamentous, and Transligamentous (rather than transverse carpal ligament) are pathways in which the thenar branch of MN passes through them to reach the thenar muscle and are explained by some authors [9, 15, 17]. Recurrent branches of MN passed through the transverse carpal ligament have critical importance in carpal tunnel release and loss of motor function in possible injuries that may lead to adverse iatrogenic morbidity [22].
PMA is the most common coexistence anomaly with MN variations reported by some authors [11, 15, 20] (Table 13).
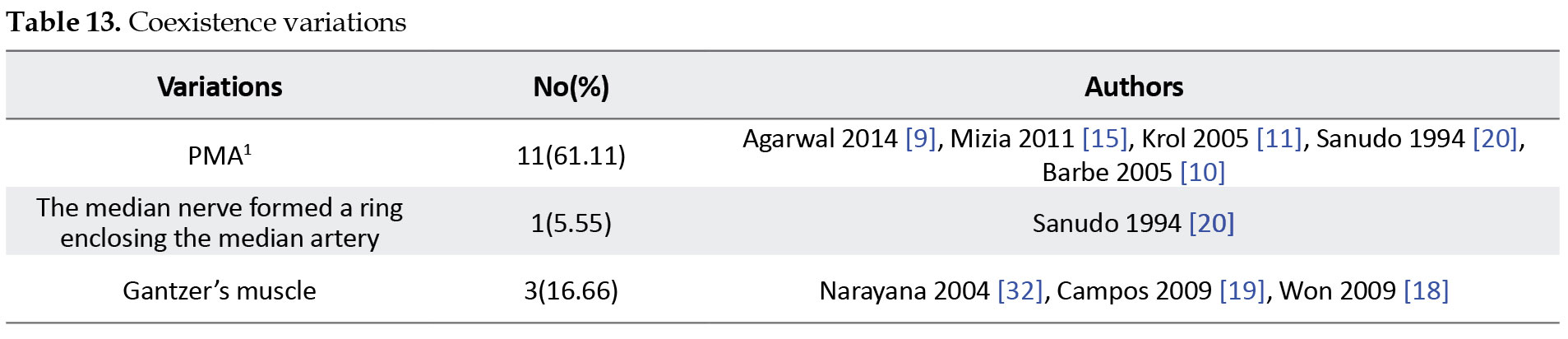
Because of the involution of PMA in embryologic life, it is not seen in adults usually [71]. However, Gassner [72] reported PMA in 16% of 100 hands studied by color Doppler ultrasonography in 50 asymptomatic volunteers. PMA is commonly associated with high division of MN [9, 10, 11, 44]. Most people with PMA seem asymptomatic [72], but some suffer from carpal tunnel syndrome secondary to PMA thrombosis [73, 74].
Incomplete superficial palmar arch is another significant coexistence anomaly, and its possible simultaneous neural variations must be considered by surgeons performing vascular grafts or repairing vascular surgeries [39]. The Gantzer’s muscle (flexor digitrum profundus with two accessory heads) and simultaneous neural variations can cause a clinical condition called anterior interosseous syndrome [75]. The knowledge of these variations reported in the paper may be helpful for all specialists concerned about MN surgery, electrophysicion, and radiologic evaluation.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
References
Lateral (C5,6,7) and medial (C8, T1) cords of brachial plexus (BP) give two main median nerve (MN) roots uniting anterior to the axillary artery to form MN [1]. This formation pattern follows the BP embryological development basis in which the upper limb buds are included in the cervicothoracic segments (C5-T1) region and develop through the upper limb mesoderm and pierces it as ventral rami of the spinal cord [2].
After forming anterolaterally to the brachial artery, MN distally runs and crosses to the medial side of the brachial artery. Interestingly, branches supplying the elbow joint are reported as a single division of MN in the arm and axilla. The medial aspect of the brachial artery and heads of pronator teres are entrance and exit points that MN passes through them within the cubital fossa. Then MN runs between flexor digitorum superficialis and profondus to hand while passes deep to Palmaris longus and flexor retinaculum. The distal edge of the flexor retinaculum is the point at which the recurrent branch derives from the lateral side of the MN trunk supplying three Thenar muscles. Then, it runs around the flexor retinaculum. After passing between the flexor pollicis brevis and abductor pollicis brevis, its pathway ends in the medial edge of the opponens pollicis muscle, and then two main ramus derive from MN. The lateral ramus (first Common Digital Nerve [CDN]) supplies the thumb and lateral side of an index by two Proper Palmar Digital Nerves (PPDN), which the nerve to the radial side of the index innervates the first lumbrical muscle. The medial ramus divides into two (second and third) CDN supplying medial aspects of the index and adjacent sides of the middle digit and lateral side of the ring digit, and the second CDN supplies the second lumbrical muscle [1, 3].
Behnejad et al. [4] studied MN variations in the proximal part of the upper limbs. However, the complications involved in MN distal to cubital fossa are common and have clinical importance; for example, entrapment of MN in the carpal tunnel is the most common entrapment neuropathy in the clinical setting [5, 6, 7]. Still, anatomical variations from unremarkable abnormality to noticeable changes with diagnostic and therapeutic clinical importance can affect every part of the human body. MN variations also are common and are investigated and reported by many authors [8, 9, 10, 11, 12, 13, 14].
This survey aims to study median nerve variations and their clinical implications in the distal part of the upper limb to help surgeons, electrophysicians, and radiologists better know MN anatomy and anomaly to decrease iatrogenic mistakes.
2. Materials and Methods
This study is based on data published about MN variation from 1990 to 2020. Pubmed, Science Direct, and Google Scholar were researched to obtain relevant data by the following keywords: “Median nerve,” “Brachial plexus,” “Carpal tunnel,” and MeSH phrases made from the terms “Variation,” and “Cadaveric study.” We limited our research to dissection investigations. After downloading articles, we again searched associated references of pieces of literature to increase our data. Case reports, multiple cadaveric studies, and review articles were chosen for this study, and we didn’t apply any limitations. After reading the full text of all papers, we classified MN variations as reported in this paper.
3. Results
We categorized MN variations and coexistence anomalies into five groups as reported. Communication between the 4th common digital nerve of UN to the 3rd CDN of MN is the most common MN variation at the distal of the upper limb. The total numbers of cases with variation in the distribution of MN are 327 cases (Table 1).
4. Discussion
MN anatomy distal to cubital fossa doesn’t wholly match with related anatomy textbooks explanations and its different anatomy reported by many authors [8, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41]. The MN anomalies have spread spectrum in type and prevalence [8, 9, 10, 13, 37]. Notably, the prevalence of variation investigated in dissection studies is more common than in surgical observation, probably because of limitations on patient dissection [10, 13, 42, 43, 44]. We mention coexistence anomalies in the separation part because MN variation can be attributed to other coexistence variations disrupting normal MN development [9, 15, 32]. Variations in the distribution of MN were reported in 252 cases, including different types of variations. Of 327 patients, 113 can be categorized in one of Lanz’s classification groups (Tables 2, 3, 4 and 5).
However, the new variations compiled from cadaveric observations can be classified into five groups:
I) Variation in the distribution of MN in palm (Table 5)
II) Variation in MN innervation pattern (Table 5)
III) Communicating branches between MN and UN in the forearm (Table 6)
IV) Communicating branches between MN and UN in palm (Tables 7, 8, 9, 10 and 11)
V) Variation in the course of MN (Table 12)
Lanz’s classification contains (Tables 2, 3 and 4):
I) Variation of thenar branch course
II) Accessory branches derived from MN at the distal of carpal tunnel
III) High division of MN
IV) Accessory branches derived from MN at the proximal part of carpal tunnel
The prevalence of MN variation described by Lanz’s groups (I-IV) were 46%, 7.5%, 2.9%, and 2.9%, respectively [13]. However, our study verifies the high prevalence of Lanz I, too.
Entrapment of MN beneath the flexor retinaculum presented by carpal tunnel syndrome, including some symptoms (such as numbness and weakness) and signs (such as Tinel sign and Phalen sign). These signs and symptoms can be alleviated by decompressing MN via endoscopic or open surgeries [45, 46, 47, 48]. Unfortunately, injury to the third common digital nerve (TCDN) is the most common post-carpal tunnel release operation complication [49]. Despite the clinical importance of the TCDN branching pattern, its variations had not been reported since Engineer et al. [14] classified variations of TCDN into three groups:
1) TCDN originates from MN proximal to the distal edge of the TCL
2) TCDN originates from MN distal to TCL but proximal to superficial palmar arch
3) TCDN originates from MN distal to TCL and superficial palmar arch
Notably, all TCDN variations may be vulnerable to damage by open carpal tunnel surgeries. Types 2 and 3 may potentially risk injury in endoscopy techniques. Despite visualization limitations, the Agee endoscopic surgery technique can preserve TCDN and its three types of variations from possible damage if done by a professional surgeon [14].
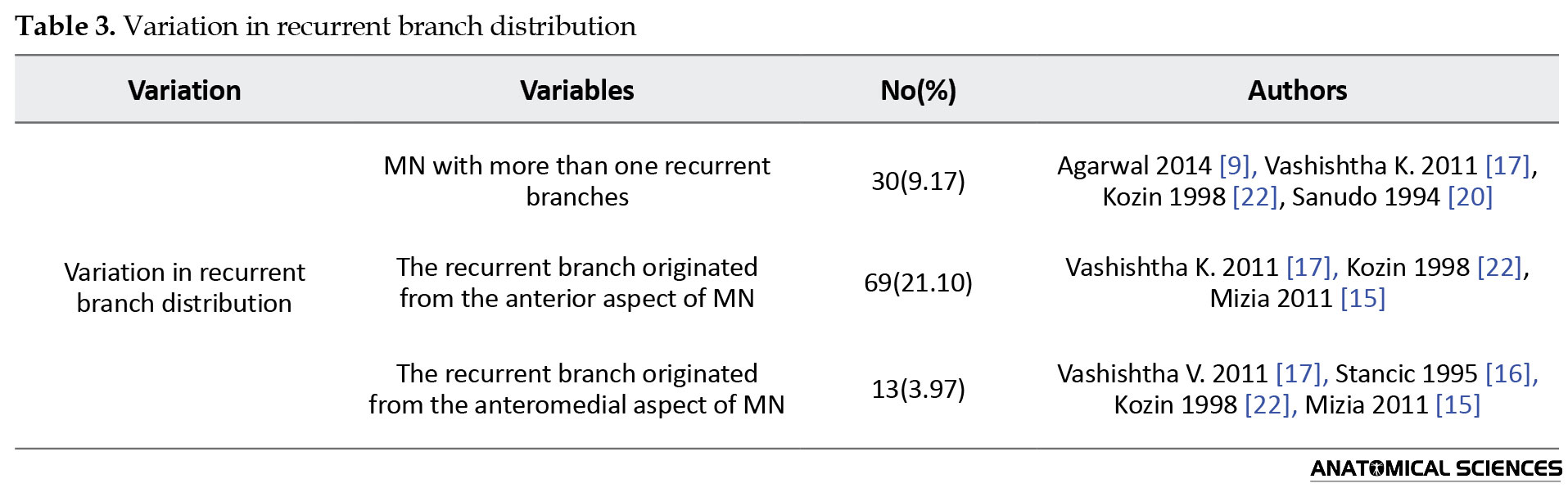
High bifurcation and trifurcation of MN are common variations of MN distribution [17]. Amadio documented high bifurcation MN in 9 cases in carpal tunnel decompression surgery [50]. Abnormal origination of recurrent branches is another variation of MN distribution, increasing the risk of MN injuries in carpal tunnel decompression [17].
Supplying all lumbricals from UN is highly associated with the presence of MGA in the forearm [23]. Originating the third lumbrical muscle nerve from MN is a rare variation reported by some authors [17, 51]. However, proximal UN injuries with incomplete clawed-hand must be considered as the presence of MGA [52]. Linell [53] reported one hand in which the UN supplied two sides of the ring finger and three hands in which the UN innervated the medial side of the middle finger. However, all variations associated with MN innervations patterns may disrupt post-trauma evaluations.
Martin-Gruber anastomosis was first described by Swedish anatomist Martin (1763) [54] and Gruber (1810) [55], is a connection between MN and UN in the forearm, and it can be classified into seven subtypes as documented in the previous part (Table 5). MGA has been seen in the primate’s elbows too. The MGA reveals a common trunk supplying the flexor compartment of the forearm in embryological life [56]. Examination of family members with MGA variations indicated some genetic features of this variation, and an Autosomal Dominant pattern was suggested for it [57]. Some hypotheses consider the role of chromosome 21 in this variation. Srinvasan and Rhodos [58] reported MGA bilaterally in fetuses carrying an extra 21 chromosomes (21 trisomies). Prevalence of MGA follows a difference statistically high prevalence of MGA was reported by Erdem et al. [59], Amoiridis [60], Lee et al. [29], and medium prevalence was reported by Shu et al. [25], and Nakashima [24] and low prevalence of this variation was documented by de Alemida et al. [61] and Prates et al. [62]. These different ranges can be explained by the different methodology used for studies and genetic variation between examined target populations [26]. Notably, MGA can change the clinical manifestations of patients suffering from pronator syndrome by changing muscle innervation patterns and sensory distribution [28, 63].
Marinacci anastomosis, called Martin-Gruber reverse anastomosis too, was first reported in a patient who presented with MN trauma, and despite forearm flexor muscle denervation, hand muscle function was normal [64]. However, communicating branch from UN to MN (Marinacci anastomosis) is a rare variation, and Kimura et al. [65] didn’t report any UN to MN communication in their electrophysiological examinations.
Palmar communication between MN and UN is the most common variation of MN and can be categorized into five subtypes as presented. Communicating branches often arose from UN to MN and were reported by some authors [23, 56, 57, 66]. However, the crucial role of these connections is in changing the pattern of sensory loss when MN or UN is compressed, which may lead to clinical mistakes [67].
Petro Berrettini [68] was the first man to paint the superficial palmar communication between UN and MN in the anatomy atlas. The Berrettini anastomosis can be categorized into three groups, as reported in the previous part (Table 4). However, some authors believed that Berretin anastomosis must be considered a normal anatomic discovery, and even in some papers, this anastomosis has been seen in all cases [69, 70].
Don Griot et al. [34] emphasized the advantage of Berretin anastomosis knowledge for surgeons performing carpal tunnel release, Dupuytren fasciotomy, and flexor tendons surgeries. Because of the high prevalence of UN and MN communications and their possible role in either diagnostic or therapeutic mistakes, some studies should be done to evaluate the relation of these variations and their potential clinical manifestation.
Subligamentous, Extraligamentous, and Transligamentous (rather than transverse carpal ligament) are pathways in which the thenar branch of MN passes through them to reach the thenar muscle and are explained by some authors [9, 15, 17]. Recurrent branches of MN passed through the transverse carpal ligament have critical importance in carpal tunnel release and loss of motor function in possible injuries that may lead to adverse iatrogenic morbidity [22].
PMA is the most common coexistence anomaly with MN variations reported by some authors [11, 15, 20] (Table 13).
Because of the involution of PMA in embryologic life, it is not seen in adults usually [71]. However, Gassner [72] reported PMA in 16% of 100 hands studied by color Doppler ultrasonography in 50 asymptomatic volunteers. PMA is commonly associated with high division of MN [9, 10, 11, 44]. Most people with PMA seem asymptomatic [72], but some suffer from carpal tunnel syndrome secondary to PMA thrombosis [73, 74].
Incomplete superficial palmar arch is another significant coexistence anomaly, and its possible simultaneous neural variations must be considered by surgeons performing vascular grafts or repairing vascular surgeries [39]. The Gantzer’s muscle (flexor digitrum profundus with two accessory heads) and simultaneous neural variations can cause a clinical condition called anterior interosseous syndrome [75]. The knowledge of these variations reported in the paper may be helpful for all specialists concerned about MN surgery, electrophysicion, and radiologic evaluation.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors equally contributed to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
References
- Standring S. Gray’s Anatomy: Anatomical basis of clinical practice. Amsterdam: Elsevier; 2020. [Link]
- Schoenwolf GC, Larsen W J, Bleyl SB, Brauer PR, Francis-West PH. Larsen’s human embryology. London: Churchill Livingstone/Elsevier; 2009. [Link]
- Tom DK, Khake SA, Belsare SM, Mutalik MM. Variation in lateral root of median nerve. International Journal of Anatomy and Research. 2018; 6(3.1):5441-4. [DOI:10.16965/ijar.2018.228]
- Behnejad M, Bakhshi Kashi M, Nikzad H, Taherian A, Loghman A. Variations of median nerve from axillary region to cubital fossa. Anatomical Sciences Journal. 2016; 13(1):3-12. [Link]
- Amadio PC. Bifid median nerve with a double compartment within the transverse carpal canal. The Journal of Hand Surgery. 1987; 12(3):366-8. [DOI:10.1016/S0363-5023(87)80005-9]
- Aydin K, Cokluk C, Piskin A, Kocabicak E. Ultrasonographically checking the sectioning of the transverse carpal ligament during carpal tunnel surgery with limited uni skin incisions. Turkish Neurosurgery. 2007; 17(3):219-23. [PMID]
- Ranjan P, Bhuiyan PS. A study of variation in median nerve formation in cadavers. International Journal of Anatomy and Research. 2020; 8(1.3):7395-8. [DOI:10.16965/ijar.2020.111]
- Mogra K, Garg R, Shekhawat S. Variance in the course of palmar cutaneous branch of median nerve along with a variant head of biceps brachii: A cadaveric case report. Journal of Evolution of Medical and Dental Sciences. 2014; 3(3):608-12. [DOI:10.14260/jemds/2014/1873]
- Agarwal P, Gupta S, Yadav P, Sharma D. Cadaveric study of anatomical variations of the median nerve and persistent median artery at wrist. Indian Journal of Plastic Surgery. 2014; 47(1):95-101. [PMID] [PMCID]
- Barbe M, Bradfield J, Donathan M, Elmaleh J. Coexistence of multiple anomalies in the carpal tunnel. Clinical Anatomy. 2005; 18(4):251-9. [DOI:10.1002/ca.20086] [PMID]
- Krol A, Palczak A, Jedrzejewski KS. Split median nerve. A report of twocases. Folia Morphologica (Warsz). 2005; 64(4):341-4. [PMID]
- Dogan NU, Uysal II, Seker M. The communications between the ulnar and median nerves in upper limb. Neuroanatomy. 2009; 8(1):15-9. [Link]
- Lanz U. Anatomical variations of the median nerve in the carpal tunnel. The Journal of Hand Surgery. 1977; 2(1):44-53. [DOI:10.1016/S0363-5023(77)80009-9]
- Engineer NJ, Hazani R, Mowlavi A, Neumeister MW, Lee WA, Wilhelmi BJ. Variations in the anatomy of the third common digital nerve and landmarks to avoid injury to the third common digital nerve with carpal tunnel release. Eplasty. 2008; 8:e51. [PMID] [PMCID]
- Mizia E, Klimek-Piotrowska W, Walocha J, Rutowski R, Wojtala R. The median nerve in the carpal tunnel. Folia Morphologica (Warsz). 2011; 70(1):41-6. [PMID]
- Stancic M, Eskinja N, Stosic A. Anatomical variations of the median nerve in the carpal tunnel. International Orthopaedics. 1995; 19(1):30-4. [DOI:10.1007/BF00184911] [PMID]
- Vashishtha K. Variations of median nerve in carpal tunnel and its distribution in hand. Journal of Anatomical Society of India. 2011; 60(2):193-8. [DOI:10.1016/S0003-2778(11)80025-0]
- Won H-S, Oh C-S, Chung I-H. A split and conjoined median nerve in the forearm. Anatomical Science International. 2010; 85(2):115-7. [DOI:10.1007/s12565-009-0040-3] [PMID]
- Campos D, Nazer M, Bartholdy L. Anatomical variation of the accessory muscle of the forearm (Gantzer’s muscles) and his relationship with the median nerve: A case report in human. Brazilian Journal of Morphological Sciences. 2009; 26(1):39-41. [Link]
- Sanudo J, Chikwe J, Evans S. Anomalous median nerve associated with persistent median artery. Journal of Anatomy. 1994; 185(2):447-51. [PMDI] [PMCDI]
- Sundaram SM, Kumar MS, Sethupathi BB, Nayak SR, Krishnamurthy A. Split median nerve with variation in its common digital branch-A case report. Neuroanatomy. 2008; 7:15-8. [Link]
- Kozin SH. The anatomy of the recurrent branch of the median nerve. The Journal of Hand Surgery. 1998; 23(5):852-8. [DOI:10.1016/S0363-5023(98)80162-7] [PMID]
- Taams K. Martin-gruber connections in south africa An anatomical study. The Journal of Hand Surgery (British and European Volume). 1997; 22(3):328-30. [DOI:10.1016/S0266-7681(97)80396-8]
- Nakashima T. An anatomic study on the Martin-Gruber anastomosis. Surgical and Radiologic Anatomy. 1993; 15(3):193-5. [DOI:10.1007/BF01627703] [PMID]
- Shu H, Chantelot C, Oberlin C, Alnot J, Shao H. Martin-Gruber communicating branch: Anatomical and histological study. Surgical and Radiologic Anatomy. 1999; 21(2):115-8. [DOI:10.1007/s00276-999-0115-9] [PMID]
- Ballesteros LE, Forero PL, Quintero ID. Median ulnar nerves communication in the forearm: A study with autopsy material. Italian Journal of Anatomy and Embryology 2014; 119(3):232-40. [PMID]
- Sarikcioglu L, Sindel M, Ozkaynak S, Aydin H. Median and ulnar nerve communication in the forearm: An anatomical andelectrophysiological study. Medical Science Monitor. 2003; 9(9):351-6. [PMID]
- Fellipe M, Telles F, Soares A, Felippe F. Anastomosis between median nerve and ulnar nerve in the forearm. Journal of Morphological Science. 2012; 29(1):23-6. [Link]
- Lee KS, Oh CS, Chung IH, Sunwoo IN. An anatomic study of the Martin-Gruber anastomosis: Electrodiagnostic implications. Muscle & Nerve. 2005; 31(1):95-7. [DOI:10.1002/mus.20141] [PMID]
- Rodriguez‐Niedenfuhr M, Vazquez T, Parkin I, Logan B, Sanudo JR. Martin-Gruber anastomosis revisited. Clinical Anatomy. 2002; 15(2):129-34. [DOI:10.1002/ca.1107] [PMID]
- Rodriguez‐Niedenfuhr M, Vazquez T, Ferreira B, Parkin I, Nearn L, Sanudo JR. Intramuscular Martin‐Gruber anastomosis. Clinical Anatomy. 2002; 15(2):135-8. [DOI:10.1002/ca.1108] [PMID]
- Narayana H, Narendiran K, Shetty KP, Prashanthi N, Narayana K. A case of coexistence of three anatomical variations in the forearm: Gantzer’s muscle, Martin-Gruber anatomosis, and nerve of Henle. European Journal of Anatomy. 2004; 8(2):81-4. [Link]
- Ajmani M. Variations in the motor nerve supply of the thenar and hypothenar muscles of the hand. The Journal of Anatomy. 1996; 189(1):145-50. [PMID] [PMCID]
- Peter J, Griot WD, Zuidam JM, Van Kooten EO, Prose LP, Hage JJ. Anatomic study of the ramus communicans between the ulnar and median nerves. The Journal of Hand Surgery. 2000; 25(5):948-54. [DOI:10.1053/jhsu.2000.16352] [PMID]
- Ferrari G, GilbertA. The superficial anastomosis on the palm of the hand between the ulnar and median nerves. The Journal of Hand Surgery (European Volume). 1991; 16(5):511-4. [DOI:10.1016/0266-7681(91)90105-W] [PMID]
- Tagil SM, Bozkurt MC, Ozcakar L, Ersoy M, Tekdemi̇r I, Elhan A. Superficial palmar communications between the ulnar and median nerves in Turkish cadavers. Clinical Anatomy. 2007; 20(7):795-8. [DOI:10.1002/ca.20517] [PMID]
- Loukas M, Louis Jr RG, Stewart L, Hallner B, DeLuca T, Morgan W, et al. The surgical anatomy of ulnar and median nerve communications in thepalmar surface of the hand. Journal of Neurosurgery. 2007; 106(5):887-93. [DOI:10.3171/jns.2007.106.5.887] [PMID]
- Griot JPWD, van Kooten EO, Zuidam JM, Prose LP, Hage JJ. Internal anatomy of the communicating branch between the ulnar and median nerves in the hand and its relevance to volar digital sensibility. The Journal of Hand Surgery. 2002; 27(1):143-6. [DOI:10.1053/jhsu.2002.30075] [PMID]
- Sirasanagandla SR, Patil J, Potu BK, Nayak BS, Shetty SD, Bhat KM. A rare anatomical variation of the Berrettini anastomosis and third common palmar digital branch of the median nerve. Anatomical Science International. 2013; 88(3):163-6. [DOI:10.1007/s12565-012-0167-5] [PMID]
- Bas H, Kleinert JM. Anatomic variations in sensory innervation of the hand and digits. The Journal of Hand Surgery. 1999; 24(6):1171-84. [DOI:10.1053/jhsu.1999.1171] [PMID]
- Kawashima T, Sato K, Sasaki H. Stratification of theflexor retinaculum and the course and distribution of the ulnar, median, and palmar digital nerves: An anatomical study. Clinical Anatomy. 2004; 17(8):643-50. [DOI:10.1002/ca.20028] [PMID]
- Vashishtha K, Kaushal S, Chhabra U. Unusual course of median nerve. International Journal of Anatomical Variations. 2010; 3:216-7. [Link]
- Naff N, Dellon A, Mackinnon S. The anatomical course of the palmar cutaneous branch of the median nerve, including a description of its own unique tunnel. The Journal of Hand Surgery: (European Volume). 1993; 18(3):316-7. [DOI:10.1016/0266-7681(93)90050-P]
- Lindley SG, Kleinert JM. Prevalence of anatomic variations encountered in elective carpal tunnel release. The Journal of Hand Surgery. 2003; 28(5):849-55. [DOI:10.1016/S0363-5023(03)00365-4]
- Anderson BA. Endoscopic carpal tunnel release: A new approach to carpaltunnel syndrome. Aorn Journal, the official Voice of Perioperative Nurses. 1993; 57(2):413-28. [DOI:10.1016/S0001-2092(07)64100-3]
- Brown MG, Keyser B, Rothenberg ES. Endoscopic carpal tunnel release. The Journal of Hand Surgery. 1992; 17(6):1009-11. [DOI:10.1016/S0363-5023(09)91047-4]
- Chow JC. Endoscopic release of the carpal ligament: A new technique for carpal tunnel syndrome. Arthroscopy. 1989; 5(1):19-24. [DOI:10.1016/0749-8063(89)90085-6]
- Nagle DJ. Endoscopic carpal tunnel release. Hand Clinics. 2002; 18(2):307-13. [DOI:10.1016/S0749-0712(02)00019-7]
- Palmer AK, Toivonen DA. Complicationsof endoscopic and open carpal tunnel release. The Journal of Hand Surgery. 1999; 24(3):561-5. [DOI:10.1053/jhsu.1999.0561] [PMID]
- Amadio PC. Anatomic variations of the median nerve within the carpal tunnel. Clinical Anatomy. 1988; 1(1):23-31. [DOI:10.1002/ca.980010106]
- Mehta H, Gardner W. A study of lumbrical muscles in the human hand. American Journal of Anatomy. 1961; 109(3):227-38. [DOI:10.1002/aja.1001090302] [PMID]
- Brandsma J, Birke J, Sims D. The Martin-Gruber innervated hand. The Journal of Hand Surgery. 1986; 11(4):536-9. [DOI:10.1016/S0363-5023(86)80193-9]
- Linell EA. The distribution of nerves in the upper limb, with reference to variabilities and their clinical significance. Journal of Anatomy. 1921; 55(2-3):79-112. [PMID] [PMCID]
- Martin R. [Speeches, on the general characteristics of nerves in the human body, given for Kongl. The Academie of Science, at præsidii closure: ... and, together with justifiable draft of the specific anatomical description of the nerves, etc. (Swedish)]. Stockholm: Lars Salvius; 1763. [Link]
- Gruber W. Ueber die Verbindung des Nervusmedianus mit dem Nervus ulnaris am Unterame des Menschen um der Saugethiere. [Archives of Anatomy and Physiology (German)] Archives of Anatomy and Physiology. 1870; 37(2):501-22. [Link]
- Iyer V, Fenichel G. Normal median nerve proximal latency in carpal tunnel syndrome: A clue to coexisting Martin-Gruber anastomosis. Journal of Neurology, Neurosurgery & Psychiatry. 1976; 39(5):449-52. [DOI:10.1136/jnnp.39.5.449] [PMID] [PMCID]
- Crutchfield CA, Gutmann L. Hereditary aspects of median-ulnar nerve communications. Journal of Neurology, Neurosurgery & Psychiatry. 1980; 43(1):53-5. [DOI:10.1136/jnnp.43.1.53] [PMID] [PMCID]
- Srinivasan R, Rhodes J. The median-ulnar anastomosis (Martin-Gruber) in normal and congenitally abnormal fetuses. Archives of Neurology. 1981; 38(7):418-9. [DOI:10.1001/archneur.1981.00510070052007] [PMID]
- Erdem HR, Ergun S, Erturk C, Ozel S. Electrophysiological evaluation of the incidence of Martin-Gruber anastomosis in healthy subjects. Yonsei Medical Journal. 2002; 43(3):291-5. [DOI:10.3349/ymj.2002.43.3.291] [PMID]
- Amoiridis G. Median-ulnar nerve communications and anomalous innervation of the intrinsic hand muscles: An electrophysiological study. Muscle & Nerve. 1992; 15(5):576-9. [DOI:10.1002/mus.880150507] [PMID]
- de Almeida JA, Vitti M, Garbino JA. [Anatomical study of Martin-Gruber anastomosis (Portugees)]. Hansenologia Internationalis. 1999; 24(1):15-20. [Link]
- Prates LC, Carvalho VCD, Prates JC, Langone F, Maretto M. The Martin-Gruber anastomosis in Brazilians. An anatomical study. Brazilian Journal of Morphological Sciences. 2003; 20(3):177-80. [Link]
- Sraj SA, Moussallem CD, Stafford JB. Cubital tunnel syndrome presenting with carpal tunnel symptoms: Clinical evidence for sensory ulnar-to-median nerve communication. American Journal of Orthopedics (Belle Mead NJ) . 2009; 38(6):104-6. [PMID]
- Marinacci A. The problem ofunusual anomalous innervation of hand muscles. the value of electrodiagnosis in its evaluation. Bulletin of the Los Angeles Neurological Society. 1964; 29:133-42. [Link]
- Kimura J, Murphy MJ, Varda DJ. Electrophysiological study of anomalous innervation of intrinsic hand muscles. Archives of Neurology. 1976; 33(12):842-4. [DOI:10.1001/archneur.1976.00500120046007] [PMID]
- Gutmann L. Median--ulnar nerve communications and carpal tunnel syndrome. Journal of Neurology, Neurosurgery & Psychiatry. 1977; 40(10):982-6. [DOI:10.1136/jnnp.40.10.982] [PMID] [PMCID]
- May J, Rosen H. Division of the sensory ramus communicans between the ulnar and median nerves: A complication following carpal tunnel release. A case report. JBJS Case Connector. 1981; (5):836-8. [DOI:10.2106/00004623-198163050-00025]
- da Cortona P. [Tabulae anatomicae (Latin)]. Human anatomy -- Atlases: Early works to 1800. Romae, Impensis Fausti Amidei bibliopolae in via Cursus. 174. [Link]
- Meals RA, Shaner M. Variations in digital sensory patterns: A study of the ulnar nerve-median nerve palmar communicating branch. Journal of Hand Surgery. 1983; 8(4):411-4. [DOI:10.1016/S0363-5023(83)80200-7] [PMID]
- Bonnel F, Vila R. Anatomical study of the ulnar nerve in the hand. The Journal of Hand Surgery (British and European Volume). 1985; 10(2):165-8. [DOI:10.1016/0266-7681(85)90007-5] [PMID]
- De Vriese B. [Recherches sur levolution des vaisseaux sanguins des membres chez lhomme (French)] [Research on the evolution of limb blood vessels in humans]. Archives de Biologie. 1902; 18:665-730.
- Gassner EM, Schocke M, Peer S, Schwabegger A, Jaschke W, BodnerG. Persistent median artery in the carpal tunnel color doppler ultrasonographic findings. Journal of Ultrasound in Medicine. 2002; 21(4):455-61. [DOI:10.7863/jum.2002.21.4.455] [PMID]
- Kele H, Verheggen R, Reimers CD. Carpal tunnel syndrome caused by thrombosis of the median artery: Importance of high-resolution ultrasonography for diagnosis: Case report. Journal of Neurosurgery. 2002; 97(2):471-3. [DOI:10.3171/jns.2002.97.2.0471] [PMID]
- Fumiere E, Dugardeyn C, Roquet M, Delcour C. US demonstration of a thrombosed persistent median artery in carpal tunnel syndrome. Journal of the Belgian Society of Radiology. 2002; 85(1):1-3. [PMID]
- Tabib W, Aboufarah F, Asselineau A. Compression of the anterior interosseous nerve by Gantzer’s muscle. Chirurgie de la Main. 2001; 20(3):241-6. [DOI:10.1016/S1297-3203(01)0004
Type of Study: Review |
Subject:
Gross Anatomy
Received: 2017/01/29 | Accepted: 2021/12/19 | Published: 2022/01/1
Received: 2017/01/29 | Accepted: 2021/12/19 | Published: 2022/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
