Sat, Apr 20, 2024
Volume 16, Issue 2 (Summer & Autumn 2019)
ASJ 2019, 16(2): 93-102 |
Back to browse issues page

Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Yousefi B, Dadseresht S, Karimi M, Esmaeili J. Effect of Gonal-F on the Rate of Endometrial Wall Thickness Changes in Ovary-Removed Rat in Presence and Absence of Human Chorionic Gonadotropin. ASJ 2019; 16 (2) :93-102
URL: http://anatomyjournal.ir/article-1-229-en.html
URL: http://anatomyjournal.ir/article-1-229-en.html



1- Department of Anatomy, School of Medicine, Semnan University of Medical Sciences, Semnan, Iran.
2- Department of Anatomical Sciences, Faculty of Medical Sciences, Baqiyatallah University of Medical Sciences, Tehran, Iran.
2- Department of Anatomical Sciences, Faculty of Medical Sciences, Baqiyatallah University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 680 kb]
(1264 Downloads)
| Abstract (HTML) (3080 Views)


Full-Text: (2768 Views)
1. Introduction
Female reproductive system consists of two ovaries, uterine tubes, uterus, vagina, and external genitalia. This system produces female gametes, provides a suitable environment for fertilization, maintains embryo, and produces self-control hormones. Uterus has thick and muscular walls consisting of three layers, as follows: 1. The layer of external connective tissue called premetrium, which is located along the ligament; 2. A very thick venose muscular layer called myometrium; 3. A mucosal layer called endometrium, covered by a simple cylindrical epithelium.
The thickness and structure of endometrium are affected by periodic changes in respect of ovarian hormones. This layer having lamina propria or endometrial stromal connective tissue, often has type III collagen fibers, abundant fibroblasts, and an underlying matter. The secreting cells of epithelium form several tubular uterine glands that penetrate the entire thickness of the endometrium. The endometrium has a basal layer adjacent to myometrium, consisting of multicellular lamina propria and a deep basal end of the uterine glands.
The most important changes in the reproduction stage relate to the endometrial glands and a functional layer consisting of spongy, low cell count, and substrate rich lamina propria. The major part of glands and epithelium are superficial. The functional layer undergoes a profound change in the menstrual cycle, but the basal layer remains almost unchanged. Two-thirds of the endometrial surface is an area that proliferates, and in the event of non-pregnancy, it eventually releasing in each cycle. This part consists of two sponge sections and superficial dense stratum. The basal layer has no monthly proliferation; however, it is the source of endometrial reconstruction after every bleeding of menstruation.
Ovulation occurs on the 14th day of secretion phase, on a typical 28-day cycle. Within 48-72 hours after ovulation, with the onset of progesterone secretion, the tissue appearance of the endometrium turns into the secretion phase; then, eosinophilic and protein-rich secretion materials are observable inside glands’ ducts. The secretion stage in the menstrual cycle is characterized by the cellular effects of estrogen and progesterone. At this stage, there is a significant reduction in the density of estrogen receptors in endometrial cells. During the secretion phase, the endometrial glands of their own glycogenic vacuoles, which on the 6th-7th day after ovulation reach the maximum secretion level, and endometrium has the most optimal conditions for the blastocyst implantation.
In blastocyst attachment, the endometrium undergoes several structural and biochemical changes that depend on the hormones and the regulation of genes expression. Morphological changes include changes in the plasma membrane [1], where the shape and configuration of the microvilli in the apical membrane and the number and depth of the connections types between the epithelial cells in the lateral membrane, are altered. Changes in the base membrane occur in the form of an increased thickness of base laminate and membrane folding and the cell skeleton [2]; this process ultimately leads to the possibility of implantation [3].
However, in the follicular period, there are sequential and consistent phenomena to produce a certain number of follicles for ovulation. These changes occur within 10 to 14 days, with hormones affecting the follicle. After the initial growth stage and other stages, the follicle eventually reaches the stage of pre-ovulation. At the end of this period, estrogen first slowly increases and reaches its peak just before ovulation. As the estrogen increases, the FSH decreases; on the contrary, LH increases uninterruptedly in the early stages and suddenly reaching its peak during the menstrual period. Fast follicular growth in the late follicular phase and the reduced amount of FSH indicate that the more follicle grows, the greater its sensitivity to FSH becomes. A candidate follicle for ovulation prevents its death by producing estrogen hormone. Increased estradiol concentration within the follicle causes the higher absorption of FSH into the follicle, resulting in increased follicular susceptibility to FSH.
When follicles grow, the ovarian field cells form the theca layer around follicles. LH binds to these cells and increases steroids. In the mid-menstrual period, much of the estradiol is secreted from a follicle that will later ovulate. Atresia occurs when the remaining follicles fail to reach maturity, during which estradiol receptor follicles lose their LH and FSH. Ovarian base tissue is not generally under the effect of atresia, as it still significantly secretes steroid. However, androgens especially androstenedione and testosterone excel estrogen and are major products of ovarian base tissues. Increasing the ovarian base tissue in the last follicular stage raises androgens in the mid-menstrual period.
This concurrency of such events prepares the endometrium for blastocyst attachment [4]. This period, so called the implantation window, lasts about 4-5 days after the progesterone secretion [5]. Many morphological changes are caused by changes in the plasma membrane and cellular skeletons, which ultimately lead to implantation [2-6]. Implantation included stages that each involve specific receptors and genes [4]. However, the progression of each stage initially depends on the proper interaction between the mother’s endometrium and embryonic cells [7].
In infertility treatment centers, the patient is exposed to sexual hormones to stimulate her ovaries to produce ovules. Several medications are used, including the most commonly used Gonal-F and Human Chorionic Gonadotropin (HCG) [8, 9]. Most of these medications affect hormone system changes and are able to increase or decrease the concentration of steroid hormones in the blood.
Gonal-F as a human follicle stimulating hormone is a DNA recombinant. It has two subunits of α and β consisting of 92 and 111 amino acids, respectively. It stimulates the growth of follicles in women without an initial ovarian defect and can promote follicle development. This medication does not contain LH hormone. HCG can be used to compensate the lack of LH, to mature the follicle and perform ovulation, after examining the patient and ensuring that the follicles have sufficiently developed.
Moreover, HCG is a glycoprotein that consists of 237 amino acids and a molecular weight of about 26 kDa. It is secreted from placenta syncytiotrophoblast cells and by binding to the LH receptor, contributes in the survival of corpus luteum, and the preservation of pregnancy. The molecule is composed of two subunits α and β. It’s α subunit is also observed in FSH, LH, and TSH hormones, but the subunit β is independent. This product is also used in the treatment of infertility caused by a poor pituitary function in men and infertility in women alone or in combination with other medications, including Gonal-F. With the imitation of natural LH peak in women, it stimulates ovulation in women and increases androgen by the testicle. Ovarian stimulation is commonly practiced in infertility clinics and Gonal-F is used at multiple and uncontrolled doses. Furthermore, no studies have explored this area. Therefore, we investigated the effect of these medications on this particular receptor which could be effective in the success of IVF (In Vitro Fertilization) and infertility treatment.
2. Materials and Methods
Given that the reproduction cycle of rat consists of 4 parts of proestrus, estrus, metestrus, and diestrus, the onset of puberty in female rats occurs at the fourth week of life as a result of LH secretion, which causes the ovule maturity. These changes in the secretion of LH occur about 8-9 days before the first prosthesis; then, the first stage of proestrus occurs. Therefore, we selected adult female rats [10].
Female reproductive system consists of two ovaries, uterine tubes, uterus, vagina, and external genitalia. This system produces female gametes, provides a suitable environment for fertilization, maintains embryo, and produces self-control hormones. Uterus has thick and muscular walls consisting of three layers, as follows: 1. The layer of external connective tissue called premetrium, which is located along the ligament; 2. A very thick venose muscular layer called myometrium; 3. A mucosal layer called endometrium, covered by a simple cylindrical epithelium.
The thickness and structure of endometrium are affected by periodic changes in respect of ovarian hormones. This layer having lamina propria or endometrial stromal connective tissue, often has type III collagen fibers, abundant fibroblasts, and an underlying matter. The secreting cells of epithelium form several tubular uterine glands that penetrate the entire thickness of the endometrium. The endometrium has a basal layer adjacent to myometrium, consisting of multicellular lamina propria and a deep basal end of the uterine glands.
The most important changes in the reproduction stage relate to the endometrial glands and a functional layer consisting of spongy, low cell count, and substrate rich lamina propria. The major part of glands and epithelium are superficial. The functional layer undergoes a profound change in the menstrual cycle, but the basal layer remains almost unchanged. Two-thirds of the endometrial surface is an area that proliferates, and in the event of non-pregnancy, it eventually releasing in each cycle. This part consists of two sponge sections and superficial dense stratum. The basal layer has no monthly proliferation; however, it is the source of endometrial reconstruction after every bleeding of menstruation.
Ovulation occurs on the 14th day of secretion phase, on a typical 28-day cycle. Within 48-72 hours after ovulation, with the onset of progesterone secretion, the tissue appearance of the endometrium turns into the secretion phase; then, eosinophilic and protein-rich secretion materials are observable inside glands’ ducts. The secretion stage in the menstrual cycle is characterized by the cellular effects of estrogen and progesterone. At this stage, there is a significant reduction in the density of estrogen receptors in endometrial cells. During the secretion phase, the endometrial glands of their own glycogenic vacuoles, which on the 6th-7th day after ovulation reach the maximum secretion level, and endometrium has the most optimal conditions for the blastocyst implantation.
In blastocyst attachment, the endometrium undergoes several structural and biochemical changes that depend on the hormones and the regulation of genes expression. Morphological changes include changes in the plasma membrane [1], where the shape and configuration of the microvilli in the apical membrane and the number and depth of the connections types between the epithelial cells in the lateral membrane, are altered. Changes in the base membrane occur in the form of an increased thickness of base laminate and membrane folding and the cell skeleton [2]; this process ultimately leads to the possibility of implantation [3].
However, in the follicular period, there are sequential and consistent phenomena to produce a certain number of follicles for ovulation. These changes occur within 10 to 14 days, with hormones affecting the follicle. After the initial growth stage and other stages, the follicle eventually reaches the stage of pre-ovulation. At the end of this period, estrogen first slowly increases and reaches its peak just before ovulation. As the estrogen increases, the FSH decreases; on the contrary, LH increases uninterruptedly in the early stages and suddenly reaching its peak during the menstrual period. Fast follicular growth in the late follicular phase and the reduced amount of FSH indicate that the more follicle grows, the greater its sensitivity to FSH becomes. A candidate follicle for ovulation prevents its death by producing estrogen hormone. Increased estradiol concentration within the follicle causes the higher absorption of FSH into the follicle, resulting in increased follicular susceptibility to FSH.
When follicles grow, the ovarian field cells form the theca layer around follicles. LH binds to these cells and increases steroids. In the mid-menstrual period, much of the estradiol is secreted from a follicle that will later ovulate. Atresia occurs when the remaining follicles fail to reach maturity, during which estradiol receptor follicles lose their LH and FSH. Ovarian base tissue is not generally under the effect of atresia, as it still significantly secretes steroid. However, androgens especially androstenedione and testosterone excel estrogen and are major products of ovarian base tissues. Increasing the ovarian base tissue in the last follicular stage raises androgens in the mid-menstrual period.
This concurrency of such events prepares the endometrium for blastocyst attachment [4]. This period, so called the implantation window, lasts about 4-5 days after the progesterone secretion [5]. Many morphological changes are caused by changes in the plasma membrane and cellular skeletons, which ultimately lead to implantation [2-6]. Implantation included stages that each involve specific receptors and genes [4]. However, the progression of each stage initially depends on the proper interaction between the mother’s endometrium and embryonic cells [7].
In infertility treatment centers, the patient is exposed to sexual hormones to stimulate her ovaries to produce ovules. Several medications are used, including the most commonly used Gonal-F and Human Chorionic Gonadotropin (HCG) [8, 9]. Most of these medications affect hormone system changes and are able to increase or decrease the concentration of steroid hormones in the blood.
Gonal-F as a human follicle stimulating hormone is a DNA recombinant. It has two subunits of α and β consisting of 92 and 111 amino acids, respectively. It stimulates the growth of follicles in women without an initial ovarian defect and can promote follicle development. This medication does not contain LH hormone. HCG can be used to compensate the lack of LH, to mature the follicle and perform ovulation, after examining the patient and ensuring that the follicles have sufficiently developed.
Moreover, HCG is a glycoprotein that consists of 237 amino acids and a molecular weight of about 26 kDa. It is secreted from placenta syncytiotrophoblast cells and by binding to the LH receptor, contributes in the survival of corpus luteum, and the preservation of pregnancy. The molecule is composed of two subunits α and β. It’s α subunit is also observed in FSH, LH, and TSH hormones, but the subunit β is independent. This product is also used in the treatment of infertility caused by a poor pituitary function in men and infertility in women alone or in combination with other medications, including Gonal-F. With the imitation of natural LH peak in women, it stimulates ovulation in women and increases androgen by the testicle. Ovarian stimulation is commonly practiced in infertility clinics and Gonal-F is used at multiple and uncontrolled doses. Furthermore, no studies have explored this area. Therefore, we investigated the effect of these medications on this particular receptor which could be effective in the success of IVF (In Vitro Fertilization) and infertility treatment.
2. Materials and Methods
Given that the reproduction cycle of rat consists of 4 parts of proestrus, estrus, metestrus, and diestrus, the onset of puberty in female rats occurs at the fourth week of life as a result of LH secretion, which causes the ovule maturity. These changes in the secretion of LH occur about 8-9 days before the first prosthesis; then, the first stage of proestrus occurs. Therefore, we selected adult female rats [10].
Animals were deeply anesthetized using a high dose of intraperitoneal injection of ketamine 45 IU and xylazine 15 IU. By surgery, we removed the left horn of uterus; then, the animals were randomly divided into three groups of experimental (n=35), sham (n=5), and control (n=5). The experimental group was divided into 7 subgroups based on the dose of Gonal-F (IU) with and without HCG, and HCG alone, titled as follows: 1. Gonal-F dosage 10 recipient group (G10); 2. Gonal-F dosage 20ESD recipient group (G20); 3. Gonal-F dosage 30ESD recipient group (G30); 4. Group receiving HCG; 5. Gonal-F dosage 10ESD recipient group with HCG (H+G10) ; 6. Gonal-F dosage 20ESD recipient group with HCG (H+G20); 7. Gonal-F dosage 30ESD recipient group with HCG (H+G30).
To the experimental groups, Gonal-F was intraperitoneally injected for 5 days with the desired dosages, and after the last dosages of Gonal-F, the HCG was injected to the specimens by the previous method. After 72 hours of the observation of vaginal plaque, animals were sacrificed. Samples were separated and the tissues were placed in 10% formalin solution. In tissue processing stage, the tissues were prepared for molding in the stages of dehydration, clarification, hydration, and impregnation. Then, the molds were ready to be cut with a microtome machine and transferred to the slide. After passing the deparaffinization step, the slides were prepared for staining by the H&E method.
The hematoxylin-eosin staining protocol was performed; the slides were first placed in xylene, then hydrated to 70% in absolute alcohol. Then, they were washed in distilled water and maintained in a jar of hematoxylin stain for 10 minutes. After that, we rinsed the specimens to make them blue. To differentiate the color, we immersed the slides in an acid alcohol container. Then, they were placed in lithium carbonate for 2 minutes to stabilize the color. After rewashing, the specimens were placed in eosin jar for 5 minutes. After rewashing with distilled water, we initiated the hydration stage. We proceeded from 70% alcohol to absolute alcohol. Finally, the slides were placed in xylene jar again. Eventually, the mounting and adhering the coverslip was performed by Entellan adhesive.
3. Results
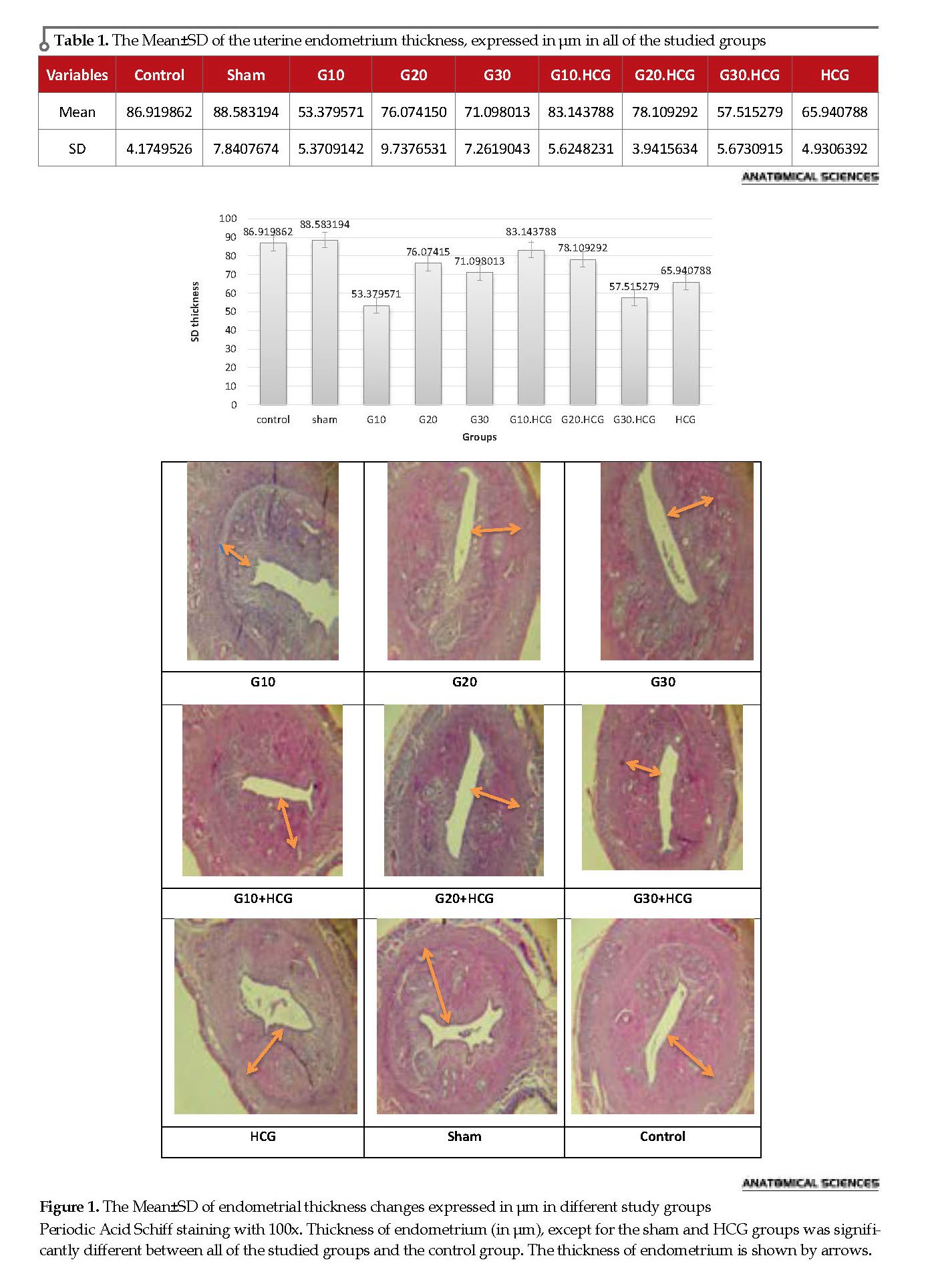
Table 1 presents the Mean±SD changes of endometrial thickness in all of the studied groups (highest thickness in G10+HCG, G20 groups). We compared the Mean±SD of endometrium thickness in μm in the studied groups. The Analysis of Variance (ANOVA) results suggested a significant difference in the endometrium thickness (in μm) between the Gonal-F recipient groups, and control, sham, and HCG groups (P<0.05) (Figure 1).
There was a significant difference between all of the groups receiving Gonal-F with the control. Endometrial thickness in the recipient groups (G10+H, G30+H, G20+H), was significantly lower than the control and sham groups (P≤0.000). There was no statistically significant difference between the G10+HCG and control group (P=0.174). The recipient groups (G10+H, G20+H) demonstrated a significant decrease compared to the control, sham and HCG groups; and a significant increase compared to G30+H group (P≤0,000). The HCG group had less increase than both control and sham groups and this difference is statistically significant (P≤0.000). In the group receiving Gonal-F and HCG, there was an increase, compared to the Gonal-F receptor group. Except for the comparison of G20 with G20+HCG which had no statistically significant difference (P=0.889), there was a significant difference between the other groups (P<0.000) (Table 2 and Figure 2).
4. Discussion
Casper et al. in 2012 investigated the association between endometrial thickness and implantation success. Their results revealed that the endometrium thickness of ˃7 mm caused the implanting embryo to be closer to the spiral arteries and oxygenated blood, and improved the possibility of further implantation [11]. Weism et al. argued that endometrium thickness of ˃14 mm clearly reduced the probability of pregnancy [12].
Richter [13] and Ai Ghamdi [14] documented that the reduced endometrium thickness decreases the probability of pregnancy. This result was confirmed by Jing Z et al. who reported that the success rate of IVF is reduced with the endometrial thickness of <7 mm [15]. Several factors change under the impression of periodic hormonal changes and hormonal treatments during assisted reproductive practices. Moreover, some factors affect the success of these treatments. In this regard, the endometrial thickness is especially important, and several researchers have addressed it [16, 17].
In the lack of intrauterine pathology, the endometrium thickness can be considered as a measure of endometrial proliferation degree. Researchers found that in the IVF cycle the endometrium thickness of at least 8 mm and a three-line pattern lead to greater success rates. Chanqq et al. investigated the effect of Gonal-F in the doses of 200-400-600 mIU/mL on endometrial cells proliferation in the culture medium, and noticed a decrease in endometrial cell proliferation [18].
Seung et al. examined the effect of FSH (5-15-30-150) IU on endometrial stromal cells in the laboratory and detected a decrease in endometrial cell proliferation [19]. Other studies have suggested that decreased endometrial cell proliferation occurs under the effect of steroid hormones, cytokines, and growth factors [20-22]. In the patients receiving Gonal-F, the estradiol level increased due to an increase in the number of follicles. Yagel stated that estradiol may negatively affect endometrial development in the follicular phase [23].
Another study found that in patients who used clomiphene citrate to treat infertility and stimulate ovulation, the success rate of pregnancy was lower, despite successful ovulation and appropriate ovules,. These researchers demonstrated that estradiol and progesterone concentrations increase and endometrial thickness decreases by using clomiphene citrate [24]. We also observed that increasing Gonal-F dose reduces the endometrium thickness. In this study, the doses of 10, 20, and 30 with HCG in rats with removed ovaries increased the endometrium thickness, which was consistent with the results of Juan Balasch and colleagues.
Among a number of patients undergoing IVF, some received Gonal-F with HCG and some others received u-FSH-HP. We found that those who received Gonal-F with HCG had more developed follicles and pregnancy rates, than those receiving u-FSH-HP [25]. Additionally, Aysin Dursun et al. injected Gonal-F in doses of 10-20 with HCG to a number of rats. They found that the mitotic index, which is a characteristic of implantation reduced in the gonadotropin receptor groups, compared to the control group. In addition, the mitotic index in the groups receiving 20 units of Gonal-F significantly reduced, compared to those receiving 10 units of that [26].
Their results were inconsistent with our findings that suggest increasing the HCG dose enhances the endometrium thickness. This needs to be further investigated. Studies have suggested that FSH, HCG, and HMG hormones increase cell proliferation due to decidualization of endometrial stromal cells [27].
In this study, HCG increased the endometrium thickness, which affirms the study of Paiva et al. who examined factors enhancing the activity of trophoblast, (Interleukin-11), factors involved in blastocyst adhesion migration (GMCF), and Fibroblast Growth Factor (FGF2). They concluded that these factors increased with HCG and endometrium thickness in its consumer groups increases accordingly [28]. Their findings were in line with our obtained data. HCG, by increasing the effect of LH through influencing LH receptor along with direct and indirect effects on the endometrium, positively affects the increased endometrium thickness and improves the implantation process.
Tesarik et al. and Rao et al. found this effect due to the impact of LH on cytokines’ regulation and growth factors production, which HCG improves the implantation by imitating such effect [29, 30]. The imitation of LH function by HCG increases the growth factors affecting the growth and development of the endometrium, which can be explained by this result. Furthermore, according to Seung et al. increasing HCG doses prevented the growth of stromal cells in the laboratory environment [19]. Check et al. found that patients with more endometrial thickness were more successful in pregnancy. They also argued that people who received clomiphene with gonadotropins had thicker endometrium than those treated with clomiphene citrate. However, both groups had less endometrial thickness than the control group [16].
The endometrium thickness in rats with removed ovaries elevates by increasing Gonal-F dose from 10 units to 20 units. Moreover, the adjunct HCG causes more thickness. However, by increasing Gonal- F with HCG from 10 units to 20 units, and from 20 units to 30 units, the thickness reduces, accordingly. Therefore, due to the high prevalence of Gonal-F in infertility treatment centers, the obtained results of this study can improve the therapeutic outcomes in clinics by changing the pharmacotherapy approach.
Ovulation stimulants are very diverse and it was not possible to study all of them in the current study. Thus, the effects of these medications, such as follitropin beta and letrozole, which are currently in use, could be further explored on the quality of endometrial factors affecting implantation. Gonal-F has been reported to change in endometrial morphology. Therefore, the effect of this medication on the morphology of epithelial cells, as an effective factors on implantation can be studied. Moreover, the impact of HCG hormone in higher doses varies with respect to the affecting factors , and can be explored in other studies.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed about the purpose of the research and its implementation stages; They were also assured about the confidentiality of their information; Moreover, They were allowed to leave the study whenever they wish, and if desired, the results of the research would be available to them.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
All authors contributed in preparing this article.
Conflict of interest
The authors declared no conflict of interest.
References
Cross JC, Werb Z, Fisher SJ. Implantation and the placenta: Key pieces of the development puzzle. Science. 1994; 266(5190):1508-18. [DOI:10.1126/science.7985020]
Navot D, Bergh Pa, Williams M, Garrlsi Gj, Guzman I, Sandler B, et al. An insight into early reproductive processes through the in vivo model of ovum donation. The Journal of Clinical Endocrinology & Metabolism. 1991; 72(2):408-14. [DOI:10.1210/jcem-72-2-408] [PMID]
Murphy CR. Uterine receptivity and the plasma membrane transformation. Cell Research. 2004; 14(4):259-67. [DOI:10.1038/sj.cr.7290227] [PMID]
Martín JC, Jasper MJ, Valbuena D, Meseguer M, Remohí J, Pellicer A, Simón C. Increased adhesiveness in cultured endometrial-derived cells is related to the absence of moesin expression. Biology of Reproduction. 2000; 63(5):1370-6. [DOI:10.1095/biolreprod63.5.1370] [PMID]
Dominguez F, Yanez-Mo M, Sanchez-Madrid F, Simon C. Embryonic implantation and leukocyte transendothelial migration: Different processes with similar players. The FASEB Journal. 2005; 19(9):1056-60. [DOI:10.1096/fj.05-3781hyp] [PMID]
CR Murph. The plasma membrane transformation of uterine epithelial cells during pregnancy. Journal of Reproduction and Fertility. 2000; 55:23-8. [PMID]
Paria BC, Reese J, Das SK, Dey SK. Deciphering the cross-talk of implantation: Advances and challenges. Science. 2002; 296(5576):2185-8. [DOI:10.1126/science.1071601] [PMID]
Branigan EF, Estes MA. Minimal stimulation IVF using clomiphene citrate and oral contraceptive pill pretreatment for LH suppression. Fertility and Sterility. 2000; 73(3):587-90. [DOI:10.1016/S0015-0282(99)00584-1]
Williams SC, G.W., Muasher SJ, Oehninger S. Minimal ovarian hyperstimulation for in vitro fertilization using sequential clomiphene citrate and gonadotropin with or without the addition of a gonadotropin-releasing hormone antagonist. Fertility and Sterility. 2002; 78(5):1068-72. [DOI:10.1016/S0015-0282(02)03374-5] [PMID]
Westwood FR. The female rat reproductive cycle: A practical histological guide to staging. Toxicologic Pathology. 2008; 36(3):375-84. [DOI:10.1177/0192623308315665] [PMID]
Casper RF. It’s time to pay attention to the endometrium. Fertility and Sterility. 2011; 96(3):519-21. [DOI:10.1016/j.fertnstert.2011.07.1096] [PMID]
Weissman A, Gotlieb L, Casper RF. The detrimental effect of increased endometrial thickness on implantation and pregnancy rates and outcome in an in vitro fertilization program. Fertility and Sterility. 1999; 71(1):147-9. [DOI:10.1016/S0015-0282(98)00413-0]
Richter KS, Bugge KR, Bromer JG, Levy MJ. Relationship between endometrial thickness and embryo implantation, based on 1,294 cycles of in vitro fertilization with transfer of two blastocyst-stage embryos. Fertility and Sterility. 2007; 87(1):53-9. [DOI:10.1016/j.fertnstert.2006.05.064] [PMID]
Al-Ghamdi A, Coskun S, Al-Hassan S, Al-Rejjal R, Awartani K. The correlation between endometrial thickness and outcome of In Vitro Fertilization and Embryo Transfer (IVF-ET) outcome. Reproductive Biology and Endocrinology. 2008; 6:37. [DOI:10.1186/1477-7827-6-37] [PMID] [PMCID]
Zhao J, Zhang Q, Li Y. The effect of endometrial thickness and pattern measured by ultrasonography on pregnancy outcomes during IVF-ET cycles. Reproductive Biology and Endocrinology. 2012; 10:100. [DOI:10.1186/1477-7827-10-100] [PMID] [PMCID]
Check JH, Nowroozi K, Choe J, Dietterich C. Influence of endometrial thickness and echo patterns on pregnancy rates during in vitro fertilization. Fertility and Sterility. 1991; 56(6):1173-5. [DOI:10.1016/S0015-0282(16)54736-0]
Schild RL, Knobloch C, Dorn C, Fimmers R, Van Der Ven H, Hansmann M. Endometrial receptivity in an in vitro fertilization program as assessed by spiral artery blood flow, endometrial thickness, endometrial volume, and uterine artery blood flow. Fertility and Sterility. 2001; 75(2):361-6. [DOI:10.1016/S0015-0282(00)01695-2]
Chang CC, Hsieh YY, Hsu KH, Lin CS. Effects of gonadotropins (Gonal-F and Puregon) on human endometrial cell proliferation in vitro. Taiwanese Journal of Obstetrics and Gynecology. 2011; 50(1):42-7. [DOI:10.3109/09513590.2010.495426] [PMID]
Ku SY, Choi YM, Suh CS, Kim SH, Kim JG, Moon SY, et al. Effect of gonadotropins on human endometrial stromal cell proliferation in vitro. Archives of Gynecology and Obstetrics. 2002; 266(4):223-8. [DOI:10.1007/s00404-002-0292-9] [PMID]
Irwin JC, Utian WH, Eckert RL. Sex steroids and growth factors differentially regulate the growth and differentiation of cultured human endometrial stromal cells. Endocrinology. 1991; 129(5):2385-92. [DOI:10.1210/endo-129-5-2385] [PMID]
Arici A, Oral E, Attar E, Tazuke SI, Olive DL. Monocyte chemotactic protein -1concentration in peritoneal fluid of woman with endometriosis. Gynecology-Endorinology. 1997; 67(6):1065-72. [PMID]
Hammond MG, Oh ST, Anners J, Surrey ES, Halme J. The effect of growth factor on the proliferation of human endometrial stromal cell in culture. Obstetrics and Gynecology. 1993; 168(4):1131-6. [PMID]
Yagel S, Ben-Chetrit A, Anteby E, Zacut D, Hochner-Celnikier D, Ron M. The effect of ethinyl estradiol on endometrial thickness and uterine volume during ovulation induction by clomiphene citrate. Fertility and Sterility. 1992; 57(1):33-6. [PMID]
Lacin S, Vatansever S, Kuscu NK, Koyuncu F, Ozbilgin K, Ceylan E. Clomiphene citrate does not affect the secretion of α3, αV and β1 integrin molecules during the implantation window in patients with unexplained infertility. Human Reproduction. 2001; 16(11):2305-9. [DOI:10.1093/humrep/16.11.2305]
Balasch J, Fábregues F, Peñarrubia J, Creus M, Vidal R, Casamitjana R, et al. Follicular development and hormonal levels following highly purified or recombinant follicle-stimulating hormone administration in ovulatory women and WHO group II anovulatory infertile patients. Journal of Assisted Reproduction and Genetics. 1998; 15(9):552-9. [DOI:10.1023/A:1022586221077] [PMID] [PMCID]
Dursun A, Sendag F, Terek MC, Yilmaz H, Oztekin K, Baka M, et al. Morphometric changes in the endometrium and serum leptin levels during the implantation period of the embryo in the rat in response to exogenous ovarian stimulation. Fertility and Sterility. 2004; 82:1121-6. [DOI:10.1016/j.fertnstert.2004.04.039] [PMID]
Tang B, Gurpide E. Direct effect of gonadotropins on decidualization of human endometrial stromal cells. The Journal of Steroid Biochemistry and Molecular Biology. 1993; 47(1-6):115-21. [DOI:10.1016/0960-0760(93)90064-4]
Paiva P, Hannan NJ, Hincks C, Meehan KL, Pruysers E, Dimitriadis E, et al. Human chorionic gonadotrophin regulates FGF2 and other cytokines produced by human endometrial epithelial cells, providing a mechanism for enhancing endometrial receptivity. Human Reproduction. 2011; 26(5):1153-62. [DOI:10.1093/humrep/der027] [PMID]
Rao C. Physiological and pathological relevance of human uterine LH/HCG receptors. Journal of the Society for Gynecologic Investigation. 2006; 13(2):77-8. [DOI:10.1016/j.jsgi.2005.12.005] [PMID]
Tesarik J, Hazout A, Mendoza C. Luteinizing hormone affects uterine receptivity independently of ovarian function. Reproductive BioMedicine Online. 2003; 7(1):59-64. [DOI:10.1016/S1472-6483(10)61729-4]
3. Results
Table 1 presents the Mean±SD changes of endometrial thickness in all of the studied groups (highest thickness in G10+HCG, G20 groups). We compared the Mean±SD of endometrium thickness in μm in the studied groups. The Analysis of Variance (ANOVA) results suggested a significant difference in the endometrium thickness (in μm) between the Gonal-F recipient groups, and control, sham, and HCG groups (P<0.05) (Figure 1).
There was a significant difference between all of the groups receiving Gonal-F with the control. Endometrial thickness in the recipient groups (G10+H, G30+H, G20+H), was significantly lower than the control and sham groups (P≤0.000). There was no statistically significant difference between the G10+HCG and control group (P=0.174). The recipient groups (G10+H, G20+H) demonstrated a significant decrease compared to the control, sham and HCG groups; and a significant increase compared to G30+H group (P≤0,000). The HCG group had less increase than both control and sham groups and this difference is statistically significant (P≤0.000). In the group receiving Gonal-F and HCG, there was an increase, compared to the Gonal-F receptor group. Except for the comparison of G20 with G20+HCG which had no statistically significant difference (P=0.889), there was a significant difference between the other groups (P<0.000) (Table 2 and Figure 2).
4. Discussion
Casper et al. in 2012 investigated the association between endometrial thickness and implantation success. Their results revealed that the endometrium thickness of ˃7 mm caused the implanting embryo to be closer to the spiral arteries and oxygenated blood, and improved the possibility of further implantation [11]. Weism et al. argued that endometrium thickness of ˃14 mm clearly reduced the probability of pregnancy [12].
Richter [13] and Ai Ghamdi [14] documented that the reduced endometrium thickness decreases the probability of pregnancy. This result was confirmed by Jing Z et al. who reported that the success rate of IVF is reduced with the endometrial thickness of <7 mm [15]. Several factors change under the impression of periodic hormonal changes and hormonal treatments during assisted reproductive practices. Moreover, some factors affect the success of these treatments. In this regard, the endometrial thickness is especially important, and several researchers have addressed it [16, 17].
In the lack of intrauterine pathology, the endometrium thickness can be considered as a measure of endometrial proliferation degree. Researchers found that in the IVF cycle the endometrium thickness of at least 8 mm and a three-line pattern lead to greater success rates. Chanqq et al. investigated the effect of Gonal-F in the doses of 200-400-600 mIU/mL on endometrial cells proliferation in the culture medium, and noticed a decrease in endometrial cell proliferation [18].
Seung et al. examined the effect of FSH (5-15-30-150) IU on endometrial stromal cells in the laboratory and detected a decrease in endometrial cell proliferation [19]. Other studies have suggested that decreased endometrial cell proliferation occurs under the effect of steroid hormones, cytokines, and growth factors [20-22]. In the patients receiving Gonal-F, the estradiol level increased due to an increase in the number of follicles. Yagel stated that estradiol may negatively affect endometrial development in the follicular phase [23].
Another study found that in patients who used clomiphene citrate to treat infertility and stimulate ovulation, the success rate of pregnancy was lower, despite successful ovulation and appropriate ovules,. These researchers demonstrated that estradiol and progesterone concentrations increase and endometrial thickness decreases by using clomiphene citrate [24]. We also observed that increasing Gonal-F dose reduces the endometrium thickness. In this study, the doses of 10, 20, and 30 with HCG in rats with removed ovaries increased the endometrium thickness, which was consistent with the results of Juan Balasch and colleagues.
Among a number of patients undergoing IVF, some received Gonal-F with HCG and some others received u-FSH-HP. We found that those who received Gonal-F with HCG had more developed follicles and pregnancy rates, than those receiving u-FSH-HP [25]. Additionally, Aysin Dursun et al. injected Gonal-F in doses of 10-20 with HCG to a number of rats. They found that the mitotic index, which is a characteristic of implantation reduced in the gonadotropin receptor groups, compared to the control group. In addition, the mitotic index in the groups receiving 20 units of Gonal-F significantly reduced, compared to those receiving 10 units of that [26].
Their results were inconsistent with our findings that suggest increasing the HCG dose enhances the endometrium thickness. This needs to be further investigated. Studies have suggested that FSH, HCG, and HMG hormones increase cell proliferation due to decidualization of endometrial stromal cells [27].
In this study, HCG increased the endometrium thickness, which affirms the study of Paiva et al. who examined factors enhancing the activity of trophoblast, (Interleukin-11), factors involved in blastocyst adhesion migration (GMCF), and Fibroblast Growth Factor (FGF2). They concluded that these factors increased with HCG and endometrium thickness in its consumer groups increases accordingly [28]. Their findings were in line with our obtained data. HCG, by increasing the effect of LH through influencing LH receptor along with direct and indirect effects on the endometrium, positively affects the increased endometrium thickness and improves the implantation process.
Tesarik et al. and Rao et al. found this effect due to the impact of LH on cytokines’ regulation and growth factors production, which HCG improves the implantation by imitating such effect [29, 30]. The imitation of LH function by HCG increases the growth factors affecting the growth and development of the endometrium, which can be explained by this result. Furthermore, according to Seung et al. increasing HCG doses prevented the growth of stromal cells in the laboratory environment [19]. Check et al. found that patients with more endometrial thickness were more successful in pregnancy. They also argued that people who received clomiphene with gonadotropins had thicker endometrium than those treated with clomiphene citrate. However, both groups had less endometrial thickness than the control group [16].
The endometrium thickness in rats with removed ovaries elevates by increasing Gonal-F dose from 10 units to 20 units. Moreover, the adjunct HCG causes more thickness. However, by increasing Gonal- F with HCG from 10 units to 20 units, and from 20 units to 30 units, the thickness reduces, accordingly. Therefore, due to the high prevalence of Gonal-F in infertility treatment centers, the obtained results of this study can improve the therapeutic outcomes in clinics by changing the pharmacotherapy approach.
Ovulation stimulants are very diverse and it was not possible to study all of them in the current study. Thus, the effects of these medications, such as follitropin beta and letrozole, which are currently in use, could be further explored on the quality of endometrial factors affecting implantation. Gonal-F has been reported to change in endometrial morphology. Therefore, the effect of this medication on the morphology of epithelial cells, as an effective factors on implantation can be studied. Moreover, the impact of HCG hormone in higher doses varies with respect to the affecting factors , and can be explored in other studies.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed about the purpose of the research and its implementation stages; They were also assured about the confidentiality of their information; Moreover, They were allowed to leave the study whenever they wish, and if desired, the results of the research would be available to them.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
All authors contributed in preparing this article.
Conflict of interest
The authors declared no conflict of interest.
References
Cross JC, Werb Z, Fisher SJ. Implantation and the placenta: Key pieces of the development puzzle. Science. 1994; 266(5190):1508-18. [DOI:10.1126/science.7985020]
Navot D, Bergh Pa, Williams M, Garrlsi Gj, Guzman I, Sandler B, et al. An insight into early reproductive processes through the in vivo model of ovum donation. The Journal of Clinical Endocrinology & Metabolism. 1991; 72(2):408-14. [DOI:10.1210/jcem-72-2-408] [PMID]
Murphy CR. Uterine receptivity and the plasma membrane transformation. Cell Research. 2004; 14(4):259-67. [DOI:10.1038/sj.cr.7290227] [PMID]
Martín JC, Jasper MJ, Valbuena D, Meseguer M, Remohí J, Pellicer A, Simón C. Increased adhesiveness in cultured endometrial-derived cells is related to the absence of moesin expression. Biology of Reproduction. 2000; 63(5):1370-6. [DOI:10.1095/biolreprod63.5.1370] [PMID]
Dominguez F, Yanez-Mo M, Sanchez-Madrid F, Simon C. Embryonic implantation and leukocyte transendothelial migration: Different processes with similar players. The FASEB Journal. 2005; 19(9):1056-60. [DOI:10.1096/fj.05-3781hyp] [PMID]
CR Murph. The plasma membrane transformation of uterine epithelial cells during pregnancy. Journal of Reproduction and Fertility. 2000; 55:23-8. [PMID]
Paria BC, Reese J, Das SK, Dey SK. Deciphering the cross-talk of implantation: Advances and challenges. Science. 2002; 296(5576):2185-8. [DOI:10.1126/science.1071601] [PMID]
Branigan EF, Estes MA. Minimal stimulation IVF using clomiphene citrate and oral contraceptive pill pretreatment for LH suppression. Fertility and Sterility. 2000; 73(3):587-90. [DOI:10.1016/S0015-0282(99)00584-1]
Williams SC, G.W., Muasher SJ, Oehninger S. Minimal ovarian hyperstimulation for in vitro fertilization using sequential clomiphene citrate and gonadotropin with or without the addition of a gonadotropin-releasing hormone antagonist. Fertility and Sterility. 2002; 78(5):1068-72. [DOI:10.1016/S0015-0282(02)03374-5] [PMID]
Westwood FR. The female rat reproductive cycle: A practical histological guide to staging. Toxicologic Pathology. 2008; 36(3):375-84. [DOI:10.1177/0192623308315665] [PMID]
Casper RF. It’s time to pay attention to the endometrium. Fertility and Sterility. 2011; 96(3):519-21. [DOI:10.1016/j.fertnstert.2011.07.1096] [PMID]
Weissman A, Gotlieb L, Casper RF. The detrimental effect of increased endometrial thickness on implantation and pregnancy rates and outcome in an in vitro fertilization program. Fertility and Sterility. 1999; 71(1):147-9. [DOI:10.1016/S0015-0282(98)00413-0]
Richter KS, Bugge KR, Bromer JG, Levy MJ. Relationship between endometrial thickness and embryo implantation, based on 1,294 cycles of in vitro fertilization with transfer of two blastocyst-stage embryos. Fertility and Sterility. 2007; 87(1):53-9. [DOI:10.1016/j.fertnstert.2006.05.064] [PMID]
Al-Ghamdi A, Coskun S, Al-Hassan S, Al-Rejjal R, Awartani K. The correlation between endometrial thickness and outcome of In Vitro Fertilization and Embryo Transfer (IVF-ET) outcome. Reproductive Biology and Endocrinology. 2008; 6:37. [DOI:10.1186/1477-7827-6-37] [PMID] [PMCID]
Zhao J, Zhang Q, Li Y. The effect of endometrial thickness and pattern measured by ultrasonography on pregnancy outcomes during IVF-ET cycles. Reproductive Biology and Endocrinology. 2012; 10:100. [DOI:10.1186/1477-7827-10-100] [PMID] [PMCID]
Check JH, Nowroozi K, Choe J, Dietterich C. Influence of endometrial thickness and echo patterns on pregnancy rates during in vitro fertilization. Fertility and Sterility. 1991; 56(6):1173-5. [DOI:10.1016/S0015-0282(16)54736-0]
Schild RL, Knobloch C, Dorn C, Fimmers R, Van Der Ven H, Hansmann M. Endometrial receptivity in an in vitro fertilization program as assessed by spiral artery blood flow, endometrial thickness, endometrial volume, and uterine artery blood flow. Fertility and Sterility. 2001; 75(2):361-6. [DOI:10.1016/S0015-0282(00)01695-2]
Chang CC, Hsieh YY, Hsu KH, Lin CS. Effects of gonadotropins (Gonal-F and Puregon) on human endometrial cell proliferation in vitro. Taiwanese Journal of Obstetrics and Gynecology. 2011; 50(1):42-7. [DOI:10.3109/09513590.2010.495426] [PMID]
Ku SY, Choi YM, Suh CS, Kim SH, Kim JG, Moon SY, et al. Effect of gonadotropins on human endometrial stromal cell proliferation in vitro. Archives of Gynecology and Obstetrics. 2002; 266(4):223-8. [DOI:10.1007/s00404-002-0292-9] [PMID]
Irwin JC, Utian WH, Eckert RL. Sex steroids and growth factors differentially regulate the growth and differentiation of cultured human endometrial stromal cells. Endocrinology. 1991; 129(5):2385-92. [DOI:10.1210/endo-129-5-2385] [PMID]
Arici A, Oral E, Attar E, Tazuke SI, Olive DL. Monocyte chemotactic protein -1concentration in peritoneal fluid of woman with endometriosis. Gynecology-Endorinology. 1997; 67(6):1065-72. [PMID]
Hammond MG, Oh ST, Anners J, Surrey ES, Halme J. The effect of growth factor on the proliferation of human endometrial stromal cell in culture. Obstetrics and Gynecology. 1993; 168(4):1131-6. [PMID]
Yagel S, Ben-Chetrit A, Anteby E, Zacut D, Hochner-Celnikier D, Ron M. The effect of ethinyl estradiol on endometrial thickness and uterine volume during ovulation induction by clomiphene citrate. Fertility and Sterility. 1992; 57(1):33-6. [PMID]
Lacin S, Vatansever S, Kuscu NK, Koyuncu F, Ozbilgin K, Ceylan E. Clomiphene citrate does not affect the secretion of α3, αV and β1 integrin molecules during the implantation window in patients with unexplained infertility. Human Reproduction. 2001; 16(11):2305-9. [DOI:10.1093/humrep/16.11.2305]
Balasch J, Fábregues F, Peñarrubia J, Creus M, Vidal R, Casamitjana R, et al. Follicular development and hormonal levels following highly purified or recombinant follicle-stimulating hormone administration in ovulatory women and WHO group II anovulatory infertile patients. Journal of Assisted Reproduction and Genetics. 1998; 15(9):552-9. [DOI:10.1023/A:1022586221077] [PMID] [PMCID]
Dursun A, Sendag F, Terek MC, Yilmaz H, Oztekin K, Baka M, et al. Morphometric changes in the endometrium and serum leptin levels during the implantation period of the embryo in the rat in response to exogenous ovarian stimulation. Fertility and Sterility. 2004; 82:1121-6. [DOI:10.1016/j.fertnstert.2004.04.039] [PMID]
Tang B, Gurpide E. Direct effect of gonadotropins on decidualization of human endometrial stromal cells. The Journal of Steroid Biochemistry and Molecular Biology. 1993; 47(1-6):115-21. [DOI:10.1016/0960-0760(93)90064-4]
Paiva P, Hannan NJ, Hincks C, Meehan KL, Pruysers E, Dimitriadis E, et al. Human chorionic gonadotrophin regulates FGF2 and other cytokines produced by human endometrial epithelial cells, providing a mechanism for enhancing endometrial receptivity. Human Reproduction. 2011; 26(5):1153-62. [DOI:10.1093/humrep/der027] [PMID]
Rao C. Physiological and pathological relevance of human uterine LH/HCG receptors. Journal of the Society for Gynecologic Investigation. 2006; 13(2):77-8. [DOI:10.1016/j.jsgi.2005.12.005] [PMID]
Tesarik J, Hazout A, Mendoza C. Luteinizing hormone affects uterine receptivity independently of ovarian function. Reproductive BioMedicine Online. 2003; 7(1):59-64. [DOI:10.1016/S1472-6483(10)61729-4]
Type of Study: Original |
Subject:
Reproductive Biology
Received: 2018/04/5 | Accepted: 2018/12/27 | Published: 2019/07/1
Received: 2018/04/5 | Accepted: 2018/12/27 | Published: 2019/07/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Contact Information
Anatomical Sciences Journal (ASJ)
Negah Institute for Scientific Communication, No.15, Na'eemi St., Mirzaye Shirazi St., Tehran, Iran.
Publisher Tel : +9821 4535 5555;
+9821 4535 5000
Website: http://www.anatomyjournal.ir/
E-mail: anatomyjournal@gmail.com
